Waist–hip ratio
Waist–hip ratio or waist-to-hip ratio (WHR) is the ratio of the circumference of the waist to that of the hips. This is calculated as waist measurement divided by hip measurement (W ÷ H). For example, a person with a 25″ (64 cm) waist and 38″ (97 cm) hips has a waist–hip ratio of about 0.66.
The WHR has been used as an indicator or measure of health, and the risk of developing serious health conditions. WHR correlates with fertility (with different optimal values for males and females).
Measurement
WHO protocol
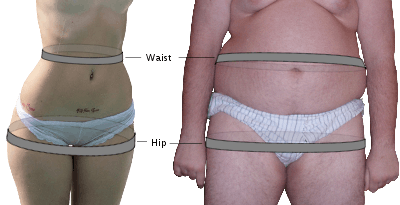
According to the World Health Organisation's data gathering protocol,[1] the waist circumference should be measured at the midpoint between the lower margin of the last palpable rib and the top of the iliac crest, using a stretch‐resistant tape that provides a constant 100 g tension. Hip circumference should be measured around the widest portion of the buttocks, with the tape parallel to the floor.[2] Other organizations use slightly different standards. The United States National Institutes of Health and the National Health and Nutrition Examination Survey used results obtained by measuring at the top of the iliac crest. Waist measurements are usually obtained by laypersons by measuring around the waist at the navel, but research has shown that these measurements may underestimate the true waist circumference.[2]
For both measurements, the individual should stand with feet close together, arms at the side and body weight evenly distributed, and should wear little clothing. The subject should be relaxed, and the measurements should be taken at the end of a normal respiration. Each measurement should be repeated twice; if the measurements are within 1 cm of one another, the average should be calculated. If the difference between the two measurements exceeds 1 cm, the two measurements should be repeated.[2]
Practical measurement
Practically, however, the waist is more conveniently measured simply at the smallest circumference of the natural waist, usually just above the belly button, and the hip circumference may likewise be measured at its widest part of the buttocks or hip.[3] Also, in case the waist is convex rather than concave, such as is the case in pregnancy, different body types, and obesity, the waist may be measured at a horizontal level 1 inch above the navel.[4]
Indicator of health
The WHR has been used as an indicator or measure of health, and the risk of developing serious health conditions. Research shows that people with "apple-shaped" bodies (with more weight around the waist) face more health risks than those with "pear-shaped" bodies who carry more weight around the hips.
WHR is used as a measurement of obesity, which in turn is a possible indicator of other more serious health conditions. The WHO states that abdominal obesity is defined as a waist–hip ratio above 0.90 for males and above 0.85 for females, or a body mass index (BMI) above 30.0.[5] The National Institute of Diabetes, Digestive and Kidney Diseases (NIDDK) states that women with waist–hip ratios of more than 0.8, and men with more than 1.0, are at increased health risk because of their fat distribution.[6]
| DGSP[7] | WHO[5] | NIDDK[6] | ||||
|---|---|---|---|---|---|---|
| Women | Men | Women | Men | Women | Men | |
| under-weight | ? | ? | ? | ? | ? | ? |
| normal weight | < 0.80 | < 0.90 | ? | ? | ? | ? |
| over-weight | 0.80–0.84 | 0.90–0.99 | ? | ? | ? | ? |
| obesity | > 0.85 | > 1.00 | > 0.85 | > 0.90 | > 0.80 | > 1.00 |
WHR has been found to be a more efficient predictor of mortality in older people (>75 years of age) than waist circumference or BMI.[8] If obesity is redefined using WHR instead of BMI, the proportion of people categorized as at risk of heart attack worldwide increases threefold.[9] The body fat percentage is considered to be an even more accurate measure of relative weight. Of these three measurements, only the waist–hip ratio takes account of the differences in body structure. Hence, it is possible for two women to have vastly different body mass indices but the same waist–hip ratio, or to have the same body mass index but vastly different waist–hip ratios.
WHR has been shown to be a better predictor of cardiovascular disease than waist circumference and body-mass index.[10] However, other studies have found waist circumference, not WHR, to be a good indicator of cardiovascular risk factors,[11] body fat distribution,[12] and hypertension in type 2 diabetes.[13]
Stress
The stress hormone cortisol is regulated by the hypothalamic-pituitary-adrenal (HPA) axis and has been associated with higher levels of abdominal fat and therefore a higher WHR.[14] Abdominal fat is a marker of visceral fat (stored around important internal organs such as the liver, pancreas and intestines) and has greater blood flow and more receptors for cortisol than peripheral fat. The greater the number of cortisol receptors, the more sensitive the visceral fat tissue is to cortisol. This heightened sensitivity to cortisol stimulates fat cells to further increase in size.[15] Women who have a combination of normal BMI and high WHR experience elevated cortisol reactivity to acute stressors and failure to habituate to repeated stressors, compared to women with normal WHR.[16] This suggests that high WHR might also indicate HPA-axis dysregulation and over-exposure to cortisol.
Evidence for the relationship between cortisol and central fat distribution has primarily been studied in individuals with Cushing’s syndrome.[17] This is characterized by over-exposure to cortisol due to elevated activity of the HPA axis. A primary component of Cushing’s syndrome is the accumulation of fat in the abdominal region, and it is hypothesized that elevated cortisol levels contribute to this accumulation. However, this hypothesis remains contested as cortisol levels only modestly explain variation in central fat distribution. It is more likely that a complex set of biological and neuroendocrine pathways related to cortisol secretion contribute to central adiposity, such as leptin, neuropeptide y, corticotropin releasing factor and the sympathetic nervous system.[17]
Growth and development
In general, adults with growth hormone deficiencies also have increased WHRs.[18][19] Adults with untreated congenital isolated growth hormone deficiency have increased WHRs, possibly from increased cortisone:cortisol ratios and insulin sensitivities.[19] Since these individuals have increased visceral obesity, it has been suggested that a minimal growth hormone secretion would theoretically increase insulin resistance.[19] However, because of the growth hormone deficiency, this insulin resistance point cannot be reached and these individuals are more sensitive to insulin. Increased adipose deposits are therefore more likely to form in these individuals, causing the high WHR. Growth hormone deficiencies have also been correlated with WHRs in prepubertal children; the specific baseline body statistics, such as WHRs, of pre-pubertal children with growth hormone deficiencies can predict growth response effectiveness to artificial growth hormone therapies, such as rhGH treatments.[20]
Sex characteristics
Males with congenital adrenal hyperplasia, determined by CYP21A2 mutations, have increased WHRs.[21]
Fertility
A WHR of 0.9 for men and 0.7 for women has been shown to correlate strongly with general health and fertility. Women within the 0.7 range have optimal levels of estrogen and are less susceptible to major diseases such as diabetes, cardiovascular disorders and ovarian cancers.[22] Women with high WHR (0.80 or higher) have significantly lower pregnancy rates than women with lower WHRs (0.70–0.79), independent of their BMIs.[23] Men with WHRs around 0.9, similarly, have been shown to be more healthy and fertile with less prostate cancer and testicular cancer.[24]
Evidence suggests that WHR is an accurate somatic indicator of reproductive endocrinological status and long-term health risk. Among girls with identical body weights, those with lower WHRs show earlier pubertal endocrine activity, as measured by high levels of lutenizing hormone and follicle-stimulating hormone, as well as sex steroid (estradiol) activity. A Dutch prospective study on outcome in an artificial insemination program provides evidence for the role of WHR and fecundity.[25] These investigators report that a 0.1 unit increase in WHR decreases the probability of conception per cycle by 30% after adjustment for age, fatness, reasons for artificial insemination, cycle length and regularity, smoking, and parity.[26][27]
Menopause, the natural or surgical cessation of the menstrual cycle, is due to an overall decrease in ovarian production of the hormones estradiol and progesterone. These hormonal changes are also associated with an increase in WHR independent of increases in body mass.[28] Significantly, studies find that large premenopausal WHRs are associated with lower estradiol levels and variation in age of menopause onset.[29] Circulating estrogen preferentially stores lipid deposits in the gluteofemoral region, including the buttocks and thighs, and evidence suggests that menopause-associated estrogen deficiency results in an accumulation of adipose deposits around the abdomen.[30] These menopause-induced changes in body fat distribution can be counteracted with hormone replacement therapy.[31] In contrast, aging males gradually accumulate abdominal fat, and hence increased WHR, in parallel with declining androgen levels.[32]
Cognitive ability
Using data from the U.S. National Center for Health Statistics, William Lassek at the University of Pittsburgh in Pennsylvania and Steven Gaulin of the University of California, Santa Barbara, found a child's performance in cognitive tests correlated to their mother's waist–hip ratio, a proxy for how much fat she stores on her hips.[33]
Children whose mothers had wide hips and a low waist–hip ratio scored highest, leading Lassek and Gaulin to suggest that fetuses benefit from hip fat, which contains long chain polyunsaturated fatty acids, critical for the development of the fetus's brain.[33] In addition, evidence suggests that children of low-WHR teens were protected from the cognitive deficits often associated with teen birth.
Human genetics
Studies in twins have suggested that between 22% and 61% of variability in waist-to-hip ratio may be accounted for by genetic factors.[34]
Measure of attractiveness
The concept and significance of WHR as an indicator of attractiveness was first theorized by evolutionary psychologist Devendra Singh at the University of Texas at Austin in 1993.[35][36] Singh argued that the WHR was a more consistent estrogen marker than the bust–waist ratio (BWR) studied at King's College, London by Dr. Glenn Wilson in the 1970s.[37][38]
Some researchers have found that the waist–hip ratio is a significant measure of female attractiveness.[39] Women with a 0.7 WHR are usually rated as more attractive by men from Indo-European cultures.[40] Preferences may vary, according to some studies,[41] ranging from 0.6 in China, South America, and some of Africa[42] to 0.8 in Cameroon and among the Hazda tribe of Tanzania,[24][43][44] with divergent preferences according to the ethnicity of the observed being noted.[45][46]
It appears that men in westernized societies are more influenced by female waist size than hip size:
"Hip size indicates pelvic size and the amount of additional fat storage that can be used as a source of energy. Waist size conveys information such as current reproductive status or health status ... in westernized societies with no risk of seasonal lack of food, the waist, conveying information about fecundity and health status, will be more important than hip size for assessing a female's attractiveness."— Journal of Biological Psychology, [47]
By western standards, women in foraging populations have high numbers of pregnancies, high parasite loads, and high caloric dependence on fibrous foods. These variables change across cultures, suggesting that
- the normal range of female WHR was often higher than in western cultures,
- what constituted locally “WHR” varied, and
- average WHR of nubile females and of females of peak fertility varied.
Thus, a WHR that indicates pubertal onset, sex, fertility, hormonal irregularities, and/or differentiates male from female in one population may not do so in another.[48]
In a series of 1993 studies done by Singh, men used WHR and overall body fat to determine a woman’s attractiveness. In his first study, men were shown a series of 12 drawings of women with various WHRs and body fat. Drawings with normal weight and a low WHR were associated with the most positive traits (i.e. attractive, sexy, intelligent and healthy). The drawings of thin female figures were not associated with any positive traits except youthfulness.[49]
Through this study, Singh suggests that males and females may have developed innate mechanisms which detect and make use of the WHR to assess how healthy an individual is and (particularly for men), infer possible mate value. Having a healthy mate improves the chances of producing offspring with inherited genetic protection from various diseases and a healthy mate is more likely to be a good parent (Hamilton & Zuk, 1982; Thornhill, 1993).[50]
Other studies discovered WHR as a signal of attractiveness as well, beyond just examining body fat and fertility. Barnaby Dixson, Gina Grimshaw, Wayne Linklater, and Alan Dixson conducted a study using eye-tracking techniques to evaluate men's fixation on digitally altered photographs of the same woman, as well as asking the men to evaluate the images based on attractiveness. What they found was while men fixated on the woman's breasts in each photo, they selected the images where the woman had a 0.7 WHR as most attractive, regardless of breast size.[51]
Furthermore, referencing a 2005 study conducted by Johnson and Tassinary looking at animated human walking stimuli, Farid Pazhoohi and James R. Liddle proposed that men do not solely use WHR to evaluate attractiveness, but also a means of sex-differentiation, with higher WHR perceived as more masculine and lower WHR as an indicator of femininity. Pazhoohi and Liddle used this idea as a possible additional explanation as to why men perceive a lower WHR as more attractive – because it relates to an expression of femininity, as opposed to masculinity and a higher WHR.[52] On this basis, it was shown that men with lower, more feminine, WHRs feel less comfortable and self-report lower body esteem and self-efficacy than men with higher, more masculine, WHRs.[53]
To enhance their perceived attractiveness, some women may artificially alter their apparent WHR. The methods include the use of a corset to reduce the waist size and hip and buttock padding to increase the apparent size of the hips and buttocks. In an earlier attempt to quantify attractiveness, corset and girdle manufacturers of the 20th century used a calculation called hip spring[54] (or hip-spring or hipspring), calculated by subtracting the waist measurement from the hip measurement. However this calculation fell into disuse because it is a poor indicator of attractiveness; for example, a hip spring of 10 inches (250 mm) would likely be considered quite attractive for an average-sized adult woman, but a child or petite woman with the same number would more likely be seen as malnourished.
WHR versus BMI attractiveness is related to fertility, not fat content. A study performed by Holliday used computer generated female body shapes to construct images which covary with real female body mass (indexed with BMI) and not with body shape (indexed with WHR), and vice versa. Twelve observers (6 male and 6 female) rated these images for attractiveness during an fMRI study. The attractiveness ratings were correlated with changes in BMI and not WHR. The results demonstrated that in addition to activation in higher visual areas, changing BMI also adjusted of the brain reward system. This shows that BMI, not WHR, modulates reward mechanisms in the brain and that this may have important implications for judgements of ideal body size in eating disordered individuals.[55]
Another study, conducted by Furnham, was used as an extension of Singh & Young's 1995 investigation. A total of 137 participants were in the study. There were 98 female participants. The age range was between 16 and 67. The majority of participants were undergraduates, and 90% were white British, the remainder being Asian (East Indian) and African. Their educational and socio-economic backgrounds (nearly all middle class) were fairly homogenous, and none had previously participated in any studies involving female body shape or attractiveness. It was predicted that the effect of breast size on judgment of attractiveness and age estimation would be dependent on overall body fat and the size of the waist-to-hip ratio.[56]
All the participants were given a booklet with eight pictures in total. Each figure was identified as heavy or slender, feminine WHR or masculine WHR, and large-breasted or small-breasted. The participants rated the figures for four personal attributes (attractiveness, healthiness, femininity, and kindness/understanding).[56]
When ratings of the figures' attractiveness were made, generally it appeared that bust size, WHR, and their weight were all important contributory elements. The female participants rated the figures with a low WHR as more attractive, healthy, feminine looking, and in the case of the heavy figure, more kind/understanding than did male participants. This is a particularly interesting finding, as most previous studies report that young women idealize female bodies solely on the basis of thinness. As far as the breast sizes of the slender figures is concerned, whether they had large or small breasts did not appear to have any effect on the ratings of attractiveness or kindness/understanding, and having larger breasts only increased the mean ratings of health and femininity very slightly. However, a heavy figure with a high WHR and a large bust was rated as the least attractive and healthy by all participants.[56]
Waist–hip ratio is also a reliable cue to one’s sex and it is hypothesized that the "individuals who represent a mismatch based on the cue provided by WHR (e.g., women with high WHRs or men with low WHRs) would likely be viewed as unattractive by the opposite sex." [57]
Food
A number of studies have been carried out with focus on food composition of diets in relation to changes in waist circumference adjusted for body mass index.
Whole-grain, ready-to-eat oat cereal diets reduce low-density lipoprotein cholesterol and waist circumference in overweight or obese adults more than low-fiber control food diets. Weight loss did not vary between groups.[58]
The mean annual change in waist circumference was more than 3 times as great for subjects in the white-bread cluster as subjects using a diet high in fruit, vegetables, reduced-fat dairy, and whole grains, and low in red and processed meat, fast food, and soda.[59]
A 2011 study suggest that dietary pattern high in fruit and dairy and low in white bread, processed meat, margarine, and soft drinks may help to prevent abdominal fat accumulation.[60]
See also
- Anogenital distance
- Body volume index
- Digit ratio
- Physical attractiveness
- Sagittal Abdominal Diameter (SAD)
- Sexual attraction
- Waist-to-height ratio
- Wasp waist
References
- ↑ "STEPwise approach to surveillance (STEPS)". World Health Organization. Retrieved March 21, 2012.
- 1 2 3 "Waist Circumference and Waist-Hip Ratio, Report of a WHO Expert Consultation" (PDF). World Health Organization. 8–11 December 2008. Retrieved March 21, 2012.
- ↑ In some places it is commonly accepted that a woman's waist is measured one inch (2.5cm) above her navel and that a man is measured one inch below his navel. Waist To Hip Calculator at University of Maryland Medical System. Retrieved Dec 2010
- ↑ Brown JE, Potter JD, Jacobs DR, Kopher RA, Rourke MJ, Barosso GM, Hannan PJ, Schmid LA (1996). "Maternal Waist-to-Hip Ratio as a Predictor of Newborn Size: Results of the Diana Project". Epidemiology. 7 (1): 62–6. doi:10.1097/00001648-199601000-00011. JSTOR 3702758. PMID 8664403.
- 1 2 http://whqlibdoc.who.int/publications/2011/9789241501491_eng.pdf
- 1 2 "Waist to Hip Ratio". freedieting.com.
- ↑ DGSP: S 1- Leitlinie Vorsorgeuntersuchung im Sport. 2007
- ↑ Price GM, Uauy R, Breeze E, Bulpitt CJ, Fletcher AE (August 2006). "Weight, shape, and mortality risk in older persons: elevated waist-hip ratio, not high body mass index, is associated with a greater risk of death". Am. J. Clin. Nutr. 84 (2): 449–60. PMID 16895897. Lay summary.
- ↑ Yusuf S, Hawken S, Ounpuu S, Bautista L, Franzosi MG, Commerford P, Lang CC, Rumboldt Z, Onen CL, Lisheng L, Tanomsup S, Wangai P, Razak F, Sharma AM, Anand SS (November 2005). "Obesity and the risk of myocardial infarction in 27,000 participants from 52 countries: a case-control study". Lancet. 366 (9497): 1640–9. doi:10.1016/S0140-6736(05)67663-5. PMID 16271645.
- ↑ Mørkedal B, Romundstad PR, Vatten LJ (2011). "Informativeness of indices of blood pressure, obesity and serum lipids in relation to ischaemic heart disease mortality: the HUNT-II study". European Journal of Epidemiology. 26 (6): 457–461. doi:10.1007/s10654-011-9572-7. ISSN 0393-2990. PMC 3115050
 . PMID 21461943.
. PMID 21461943. - ↑ Dobbelsteyn CJ, Joffres MR, MacLean DR, Flowerdew G (May 2001). "A comparative evaluation of waist circumference, waist-to-hip ratio and body mass index as indicators of cardiovascular risk factors. The Canadian Heart Health Surveys". Int. J. Obes. Relat. Metab. Disord. 25 (5): 652–61. doi:10.1038/sj.ijo.0801582. PMID 11360147.
- ↑ Ketel IJ, Volman MN, Seidell JC, Stehouwer CD, Twisk JW, Lambalk CB (June 2007). "Superiority of skinfold measurements and waist over waist-to-hip ratio for determination of body fat distribution in a population-based cohort of Caucasian Dutch adults". Eur. J. Endocrinol. 156 (6): 655–61. doi:10.1530/EJE-06-0730. PMID 17535865.
- ↑ Picon PX, Leitão CB, Gerchman F, Azevedo MJ, Silveiro SP, Gross JL, Canani LH (April 2007). "[Waist measure and waist-to-hip ratio and identification of clinical conditions of cardiovascular risk: multicentric study in type 2 diabetes mellitus patients]". Arq Bras Endocrinol Metabol (in Portuguese). 51 (3): 443–9. PMID 17546244.
- ↑ Wardle, J; Chida, Y; Gibson, EL; Whitaker, KL; Steptoe, A (2011). "Stress and adiposity: a meta-analysis of longitudinal studies". Obesity. 19 (4): 771–778. doi:10.1038/oby.2010.241. PMID 20948519.
- ↑ Pedersen, SB; Jonler, M; Richelsen, B (1994). "Characterization of regional and gender differences in glucocorticoid receptors and lipoprotein lipase activity in human adipose tissue. Journal of Clinical Endocrinology and Metabolism". Journal of Clinical Endocrinology and Metabolism. 78 (1): 1354–1359.
- ↑ Epel, ES; McEwen, B; Seeman, T; Matthews, K; Castellazzo, G; Brownell, KD (2007). "Stress and body shape: stress-induced cortisol secretion is consistently greater among women with central fat". Psychosomatic Medicine. 62 (5): 623–632. PMID 11020091.
- 1 2 Samaras, K; Campbell, LV (1997). "The non-genetic determinants of central adiposity". International Journal of Obesity and Related Metabolic Disorders : Journal of the International Association for the Study of Obesity. 21 (10): 839–845. doi:10.1038/sj.ijo.0800502.
- ↑ Murray, R (2010). "Partial growth hormone deficiency is associated with an adverse cardiovascular risk profile and increased carotid intima-medial thickness". Clinical Endocrinology (Oxford). 73 (4): 508–515.
- 1 2 3 Gomes-Santos, E (2014). "Increased visceral adiposity and cortisol to cortisone ratio in adults with congenital isolated GH deficiency.". Journal of Clinical Endocrinology. 99 (9): 3285–3289. doi:10.1210/jc.2014-2132.
- ↑ Esen, I (2013). "The association between growth response to growth hormone and baseline body composition of children with growth hormone deficiency". Growth Hormone and IGF Research. 23 (5): 196–199. doi:10.1016/j.ghir.2013.07.001. PMID 23890535.
- ↑ Falhammer, H (2011). "Cardiovascular risk, metabolic profile, and body composition in adult males with congenital adrenal hyperplasia due to 21-hydroxylase deficiency". European Journal of Endocrinology. 164 (2): 285–293. doi:10.1530/EJE-10-0877. PMID 21098686.
- ↑ "The Rules of Attraction in the Game of Love".
- ↑ Singh D (December 2002). "Female mate value at a glance: relationship of waist-to-hip ratio to health, fecundity and attractiveness" (PDF). Neuro Endocrinol. Lett. 23. Suppl 4: 81–91. PMID 12496738.
- 1 2 Marlowe, F; Apicella, C; Reed, D (2005). "Men's preferences for women's profile waist-to-hip ratio in two societies" (PDF). Evolution and Human Behavior. 26 (6): 458–68. doi:10.1016/j.evolhumbehav.2005.07.005.
- ↑ Zaadstra BM, Seidell JC, Van Noord PA, te Velde ER, Habbema JD, Vrieswijk B, Karbaat J (1993). "Fat and female fecundity: prospective study of effect of body fat distribution on conception rates". BMJ. 306 (6876): 484–487. doi:10.1136/bmj.306.6876.484. PMC 1676805. PMID 8448457.
- ↑ Singh (1993a). "Adaptive significance of female physical attractiveness: Role of the waist-to-hip ratio". Journal of Personality and Social Psychology. 65 (2): 293–307. doi:10.1037/0022-3514.65.2.293. PMID 8366421.
- ↑ Singh (1993b). "Body shape and women's attractiveness. The critical role of waist-to-hip ratio". Human Nature. 4 (3): 297–321. doi:10.1007/bf02692203. PMID 24214368.
- ↑ Cagnacci, A; Zanin, R; Cannoletta, M; Generali, M; Caretto, S; Volpe, A (2007). "Menopause, estrogens, progestins, or their combination on body weight and anthropometric measure". Fertility and Sterility. 88 (6): 1603–1608. doi:10.1016/j.fertnstert.2007.01.039. PMID 17481628.
- ↑ Freeman, EW; Sammel, MD; Lin, H; Gracia, CR (2007). "Obesity and reproductive hormone levels in the transition to menopause". Menopause. 17 (4): 718–726. doi:10.1097/gme.0b013e3181cec85d. PMID 20216473.
- ↑ Cagnacci et al., 2007
- ↑ Genazzani, AR; Gambacciani, M (2006). "Effect of climacteric transition and hormone replacement therapy on body weight and body fat distribution". Gynecological Endocrinology. 22 (3): 145–150. doi:10.1080/09513590600629092. PMID 16835076.
- ↑ Samaras, K; Campbell, LV (1997). "The non-genetic determinants of central adiposity". International Journal of Obesity and Related Metabolic Disorders: Journal of the International Association for the study of Obesity. 21 (10): 839–845. doi:10.1038/sj.ijo.0800502.
- 1 2 Lassek, W.; Gaulin S. (January 2008). "Waist-hip ratio and cognitive ability: is gluteofemoral fat a privileged store of neurodevelopmental resources?". Evolution and Human Behavior. 29 (1): 26–34. doi:10.1016/j.evolhumbehav.2007.07.005.
- ↑ "'Pear shaped' genes found – NHS Choices – Health News". www.nhs.uk.
- ↑ Singh D (August 1993). "Adaptive significance of female physical attractiveness: role of waist-to-hip ratio". J Pers Soc Psychol. 65 (2): 293–307. doi:10.1037/0022-3514.65.2.293. PMID 8366421.
- ↑ Buss, David. The Evolution of Desire: Strategies of Human Mating (hardcover) (second ed.). New York: Basic Books. p. 56.
- ↑ Wilson, Glenn D.; Brazendale, Anthony H. (1974). "Psychological correlates of sexual attractiveness: An empirical demonstration of denial and fantasy gratification phenomena?". Social Behavior and Personality: an international journal. 2: 30–4. doi:10.2224/sbp.1974.2.1.30.
- ↑ Wilson, Glenn; Nias, David; Brazendale, Anthony (1975). "Vital Statistics, Perceived Sexual Attractiveness, and Response to Risque Humor". The Journal of Social Psychology. 95 (2): 201–5. doi:10.1080/00224545.1975.9918705.
- ↑ Perfect waist-to-hip ratio is 0.7
- ↑ Singh, Devendra; Young, Robert K. (2001-06-27). "Body Weight, Waist-to-Hip Ratio, Breasts, and Hips: Role in Judgments of Female Attractiveness and Desirability for Relationships" (PDF). Ethology and Sociobiology. 16 (6): 483–507. doi:10.1016/0162-3095(95)00074-7.
- ↑ Fisher ML, Voracek M (June 2006). "The shape of beauty: determinants of female physical attractiveness". J Cosmet Dermatol. 5 (2): 190–4. doi:10.1111/j.1473-2165.2006.00249.x. PMID 17173598.
- ↑ Dixson BJ, Dixson AF, Li B, Anderson MJ (January 2007). "Studies of human physique and sexual attractiveness: sexual preferences of men and women in China". Am J Hum Biol. 19 (1): 88–95. doi:10.1002/ajhb.20584. PMID 17160976.
- ↑ Marlowe, F.; Wetsman, A. (2001). "Preferred waist-to-hip ratio and ecology" (PDF). Personality and Individual Differences. 30 (3): 481–489. doi:10.1016/S0191-8869(00)00039-8.
- ↑ Dixson BJ, Dixson AF, Morgan B, Anderson MJ (June 2007). "Human physique and sexual attractiveness: sexual preferences of men and women in Bakossiland, Cameroon". Arch Sex Behav. 36 (3): 369–75. doi:10.1007/s10508-006-9093-8. PMID 17136587.
- ↑ Freedman RE, Carter MM, Sbrocco T, Gray JJ (August 2007). "Do men hold African-American and Caucasian women to different standards of beauty?". Eat Behav. 8 (3): 319–33. doi:10.1016/j.eatbeh.2006.11.008. PMC 3033406. PMID 17606230.
- ↑ Freedman RE, Carter MM, Sbrocco T, Gray JJ (July 2004). "Ethnic differences in preferences for female weight and waist-to-hip ratio: a comparison of African-American and White American college and community samples". Eat Behav. 5 (3): 191–8. doi:10.1016/j.eatbeh.2004.01.002. PMID 15135331.
- ↑ Rozmus-Wrzesinska M, Pawlowski B (March 2005). "Men's ratings of female attractiveness are influenced more by changes in female waist size compared with changes in hip size". Biol Psychol. 68 (3): 299–308. doi:10.1016/j.biopsycho.2004.04.007. PMID 15620796.
- ↑ Buss, David M. (2005-07-15). The Handbook of Evolutionary Psychology. John Wiley & Sons. ISBN 9780471727224.
- ↑ Singh, Devendra (1994-01-01). "Is thin really beautiful and good? Relationship between waist-to-hip ratio (WHR) and female attractiveness". Personality and Individual Differences. 16 (1): 123–132. doi:10.1016/0191-8869(94)90116-3.
- ↑ Singh, Devendra; Young, Robert K. (1995-11-01). "Body weight, waist-to-hip ratio, breasts, and hips: Role in judgments of female attractiveness and desirability for relationships". Ethology and Sociobiology. 16 (6): 483–507. doi:10.1016/0162-3095(95)00074-7.
- ↑ Dixson, Barnaby J.; Grimshaw, Gina M.; Linklater, Wayne L.; Dixson, Alan F. (2011-02-01). "Eye-tracking of men's preferences for waist-to-hip ratio and breast size of women". Archives of Sexual Behavior. 40 (1): 43–50. doi:10.1007/s10508-009-9523-5. ISSN 1573-2800. PMID 19688590.
- ↑ Pazhoohi, F., & Liddle, J. R. (2012). IDENTIFYING FEMININE AND MASCULINE RANGES FOR WAIST-TO-HIP RATIO. Journal Of Social, Evolutionary & Cultural Psychology, 6(2), 227-232.
- ↑ Pazhoohi, F., Hosseinchari, M., and Doyle J. F. (2012). Iranian men’s waist-to-hip ratios, shoulder-to-hip ratios, body esteem and self-efficacy. Journal of Evolutionary Psychology. 10(2), 61–67.
- ↑ "Bald". corsetiere.net.
- ↑ Holliday I. E.; Longe O. A.; Thai N.; Hancock P. B.; Tovée M. J. (2011). "BMI not WHR modulates BOLD fMRI responses in a sub-cortical reward network when participants judge the attractiveness of human female bodies". PLoS ONE. 6 (11): 11. doi:10.1371/journal.pone.0027255.
- 1 2 3 Furnham, Adrian, Melanie Dias, and Alastair McClelland. "The Role of Body Weight, Waist-to-Hip Ratio, and Breast Size in Judgments of Female Attractiveness – Springer." Sex Roles 39.3-4 (n.d.): 311-26.
- ↑ Pazhoohi F, Liddle JR (June 2012). "Identifying feminine and masculine ranges for Waist-to-Hip ratio". Journal of Social, Evolutionary, and Cultural Psychology. 6 (2): 227–232. doi:10.1037/h0099212.
- ↑ Maki KC, Beiseigel JM, Jonnalagadda SS, Gugger CK, Reeves MS, Farmer MV, Kaden VN, Rains TM (2010). "Whole-grain ready-to-eat oat cereal, as part of a dietary program for weight loss, reduces low-density lipoprotein cholesterol in adults with overweight and obesity more than a dietary program including low-fiber control foods". Journal of the American Dietetic Association. 110 (2): 205–14. doi:10.1016/j.jada.2009.10.037. PMID 20102847.
- ↑ Newby PK, Muller D, Hallfrisch J, Qiao N, Andres R, Tucker KL (2003). "Dietary patterns and changes in body mass index and waist circumference in adults". The American Journal of Clinical Nutrition. 77 (6): 1417–25. PMID 12791618.
- ↑ Romaguera D, Ängquist L, Du H, Jakobsen MU, Forouhi NG, Halkjær J, Feskens EJ, van der A DL, Masala G, Steffen A, Palli D, Wareham NJ, Overvad K, Tjønneland A, Boeing H, Riboli E, Sørensen TI (2011). "Food composition of the diet in relation to changes in waist circumference adjusted for body mass index". PLoS ONE. 6 (8): e23384. doi:10.1371/journal.pone.0023384. PMC 3157378. PMID 21858094.
Further reading
- Karremans J. C., Frankenhuis W. E., Arons S. (2010), "Blind men prefer a low waist-to-hip ratio", Evolution and Human Behavior, 31: 182–186; doi:10.1016/j.evolhumbehav.2009.10.001.
External links
- "Waist-hip ratio should replace body mass index as indicator of mortality risk in older people" – EurekAlert August 8, 2006