Vertically transmitted infection
| Vertically transmitted infection | |
|---|---|
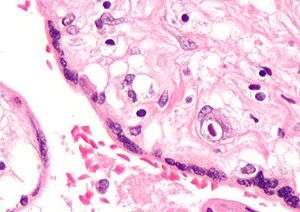 | |
| Micrograph of cytomegalovirus (CMV) infection of the placenta (CMV placentitis), a vertically transmitted infection: The characteristic large nucleus of a CMV-infected cell is seen off-centre at the bottom-right of the image, H&E stain. | |
| Classification and external resources | |
| Specialty | pediatrics |
| ICD-10 | P35-P39 |
| ICD-9-CM | 771 |
A vertically transmitted infection is an infection caused by pathogens (such as bacteria and viruses) that uses mother-to-child transmission, that is, transmission directly from the mother to an embryo, fetus, or baby during pregnancy or childbirth. It can occur when the mother gets an infection as an intercurrent disease in pregnancy. Nutritional deficiencies may exacerbate the risks of perinatal infection.
Classification
A vertically transmitted infection can be called a perinatal infection if it is transmitted in the perinatal period, which is the period starting at a gestational age of 22 weeks[1] to 28[2] (with regional variations in the definition) and ending seven completed days after birth.[1]
The term congenital infection can be used if the vertically transmitted infection persists after childbirth.
Examples
Bacteria, viruses, and other organisms are able to be passed from mother to child. Several vertically transmitted infections are included in the TORCH complex, which stands for:
- T – Toxoplasmosis / Toxoplasma gondii
- O – Other infections (see below)
- R – Rubella
- C – Cytomegalovirus
- H – Herpes simplex virus-2 or neonatal herpes simplex
The "other agents" under O include:
- Human T-lymphotropic virus[6]
- Syphilis[7]
- Zika fever, caused by Zika virus, can cause microcephaly and other brain defects in the child.[8]
Hepatitis B may also be classified as a vertically transmitted infection, but the hepatitis B virus is a large virus and does not cross the placenta, hence it cannot infect the fetus unless breaks in the maternal-fetal barrier have occurred, such as can occur in bleeding during childbirth or amniocentesis.[9]
The TORCH complex was originally considered to consist of the four conditions mentioned above,[10] with the "TO" referring to Toxoplasma. The four-term form is still used in many modern references,[11] and the capitalization "ToRCH" is sometimes used in these contexts.[12] The acronym has also been listed as TORCHES, for TOxoplasmosis, Rubella, Cytomegalovirus, HErpes simplex, and Syphilis.
A further expansion of this acronym, CHEAPTORCHES, was proposed by Ford-Jones and Kellner in 1995:[13]
- C – Chickenpox and shingles
- H – Hepatitis, C[14] (D), E
- E – Enteroviruses
- A – AIDS (HIV infection)
- P – Parvovirus B19 (produces Hydrops faetalis secondary to aplastic anemia)
- T – Toxoplasmosis
- O – Other (Group B Streptococcus, Listeria, Candida, Lyme disease)
- R – Rubella
- C – Cytomegalovirus
- H – Herpes simplex
- E – Everything else sexually transmitted (gonorrhea, Chlamydia infection, Ureaplasma urealyticum, human papillomavirus)
- S – Syphilis
Signs and symptoms
The signs and symptoms of a vertically transmitted infection depend on the individual pathogen. It may cause subtle signs such as a influenza-like illness and may not even be noticed by the mother during the pregnancy. In such cases, the effects may be seen first at birth.
Symptoms of a vertically transmitted infection may include fever and flu like symptoms. The newborn is often small for gestational age. A petechial rash on the skin may be present, with small reddish or purplish spots due to bleeding from capillaries under the skin. An enlarged liver and spleen (hepatosplenomegaly) is common, as is jaundice. However, jaundice is less common in hepatitis B because a newborn's immune system is not developed well enough to mount a response against liver cells, as would normally be the cause of jaundice in an older child or adult. Hearing impairment, eye problems, mental retardation, autism, and death can be caused by vertically transmitted infections. The mother often has a mild infection with few or no symptoms.
The genetic conditions of Aicardi-Goutieres syndrome are possibly present in a similar manner.[15][16]
Routes
The main routes of transmission of vertically transmitted infections are across the placenta (transplacental) and across the female reproductive tract during childbirth.
Transplacental
The embryo and fetus have little or no immune function. They depend on the immune function of their mother. Several pathogens can cross the placenta and cause (perinatal) infection. Often, microorganisms that produce minor illness in the mother are very dangerous for the developing embryo or fetus. This can result in spontaneous abortion or major developmental disorders. For many infections, the baby is more at risk at particular stages of pregnancy. Problems related to perinatal infection are not always directly noticeable.
During childbirth
Babies can also become infected by their mothers during birth. Some infectious agents may be transmitted to the embryo or fetus in the uterus, while passing through the birth canal, or even shortly after birth. The distinction is important because when transmission is primarily during or after birth, medical intervention can help prevent infections in the infant.
During birth, babies are exposed to maternal blood, body fluids, and to the maternal genital tract without the placental barrier intervening. Because of this, blood-borne microorganisms (hepatitis B, HIV), organisms associated with sexually transmitted disease (e.g., Neisseria gonorrhoeae and Chlamydia trachomatis), and normal fauna of the genitourinary tract (e.g., Candida albicans) are among those commonly seen in infection of newborns.
Pathophysiology
Virulence versus symbiosis
In the spectrum of optimal virulence, vertical transmission tends to evolve benign symbiosis. It is, therefore, a critical concept for evolutionary medicine. Because a pathogen's ability to pass from parent to child depends significantly on the hosts' ability to reproduce, pathogens' transmissibility tends to be inversely related with their virulence. In other words, as pathogens become more harmful to, and thus decrease the reproduction rate of, their host organism, they are less likely to be passed on to the hosts' offspring, since they will have fewer offspring.[17]
Although AIDS is sometimes transmitted through perinatal transmission, its virulence can be accounted for because its primary mode of transmission is not vertical. Moreover, medicine has further decreased the frequency of vertical transmission of AIDS. The incidence of perinatal AIDS cases in the United States has declined as a result of the implementation of recommendations on HIV counselling and voluntary testing practices and the use of zidovudine therapy by providers to reduce perinatal HIV transmission.[18]
The price paid in the evolution of symbiosis is, however, great: for many generations, almost all cases of vertical transmission will continue to be pathological—in particular if any other routes of transmission exist. Many generations of random mutation and selection are needed to evolve symbiosis. During this time, the vast majority of vertical transmission cases exhibit the initial virulence.
In dual inheritance theory, vertical transmission refers to the passing of cultural traits from parents to children.[19]
Diagnosis
When physical examination of the newborn shows signs of a vertically transmitted infection, the examiner may test blood, urine, and spinal fluid for evidence of the infections listed above. Diagnosis can be confirmed by culture of one of the specific pathogens or by increased levels of IgM against the pathogen.
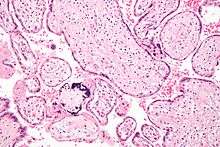 CMV placentitis
CMV placentitis CMV placentitis
CMV placentitis
Treatment and prevention

Some vertically transmitted infections, such as toxoplasmosis and syphilis, can be effectively treated with antibiotics if the mother is diagnosed early in her pregnancy. Many viral vertically transmitted infections have no effective treatment, but some, notably rubella and varicella-zoster, can be prevented by vaccinating the mother prior to pregnancy.
If the mother has active herpes simplex (as may be suggested by a pap test), delivery by Caesarean section can prevent the newborn from contact, and consequent infection, with this virus.
IgG2 antibody may play crucial role in prevention of intrauterine infections and extensive research is going on for developing IgG2-based therapies for treatment and vaccination.[20]
Prognosis
Each type of vertically transmitted infection has a different prognosis. The stage of the pregnancy at the time of infection also can change the effect on the newborn.
See also
- Group B streptococcal infection
- Susceptibility and severity of infections in pregnancy
- Horizontal disease transmission
References
- 1 2 Definitions and Indicators in Family Planning. Maternal & Child Health and Reproductive Health. By European Regional Office, World Health Organization. Revised March 1999 & January 2001. In turn citing: WHO Geneva, WHA20.19, WHA43.27, Article 23
- ↑ Singh, Meharban (2010). Care of the Newborn. p. 7. Edition 7. ISBN 9788170820536
- ↑ Yu, Jialin; Wu, Shixiao; Li, Fang; Hu, Linyan (2009). "Vertical Transmission of Chlamydia trachomatis in Chongqing China". Current Microbiology. 58 (4): 315–320. doi:10.1007/s00284-008-9331-5. ISSN 0343-8651. PMID 19123031.
- ↑ Ugen, K E; Goedert, J J; Boyer, J; et al. (June 1992). "Vertical transmission of human immunodeficiency virus (HIV) infection. Reactivity of maternal sera with glycoprotein 120 and 41 peptides from HIV type 1.". Journal of Clinical Investigation. 89 (6): 1923–1930. doi:10.1172/JCI115798. ISSN 0021-9738. PMC 295892
 . PMID 1601999.
. PMID 1601999. - ↑ Fawzi, Wafaie W.; Msamanga, Gernard; Hunter, David; et al. (2000). "Randomized Trial of Vitamin Supplements in Relation to Vertical Transmission of HIV-1 in Tanzania". Journal of Acquired Immune Deficiency Syndromes. 23 (3): 246–254. doi:10.1097/00042560-200003010-00006. ISSN 1525-4135. PMID 10839660.
- ↑ Hisada, Michie; Maloney, Elizabeth M.; Sawada, Takashi; et al. (2002). "Virus Markers Associated with Vertical Transmission of Human T Lymphotropic Virus Type 1 in Jamaica". Clinical Infectious Diseases. 34 (12): 1551–1557. doi:10.1086/340537. ISSN 1058-4838. PMID 12032888.
- ↑ Lee, M.-J.; Hallmark, R.J.; Frenkel, L.M.; Del Priore, G. (1998). "Maternal syphilis and vertical perinatal transmission of human immunodeficiency virus type-1 infection". International Journal of Gynecology & Obstetrics. 63 (3): 247–252. doi:10.1016/S0020-7292(98)00165-9. ISSN 0020-7292. PMID 9989893.
- ↑ "CDC Concludes Zika Causes Microcephaly and Other Birth Defects". CDC Newsroom Releases. Centers for Disease Control and Prevention. 13 April 2016.
- ↑ "Hepatitis B". Emergencies preparedness, response. World Health Organization. Retrieved 29 April 2016.
- ↑ Kinney, JS; Kumar, ML (December 1988). "Should we expand the TORCH complex? A description of clinical and diagnostic aspects of selected old and new agents". Clinics in perinatology. 15 (4): 727–44. ISSN 0095-5108. PMID 2850128.
- ↑ Abdel-Fattah, Sherif A.; Bhat, Abha; Illanes, Sebastian; et al. (November 2005). "TORCH test for fetal medicine indications: only CMV is necessary in the United Kingdom". Prenatal Diagnosis. 25 (11): 1028–1031. doi:10.1002/pd.1242. ISSN 0197-3851. PMID 16231309.
- ↑ Li, Ding; Yang, Hao; Zhang, Wen-Hong; et al. (2006). "A Simple Parallel Analytical Method of Prenatal Screening". Gynecologic and Obstetric Investigation. 62 (4): 220–225. doi:10.1159/000094092. ISSN 1423-002X. PMID 16791006.
- ↑ Ford-Jones, E. L.; Kellner, J. D. (1995). ""Cheap torches": An acronym for congenital and perinatal infections". The Pediatric Infectious Disease Journal. 14 (7): 638–640. doi:10.1097/00006454-199507000-00028. PMID 7567307.
- ↑ Tosone, G.; Maraolo, A.E.; Mascolo, S.; et al. (2014). "Vertical hepatitis C virus transmission: Main questions and answers". World Journal of Hepatology. 6 (8): 538–548. doi:10.4254/wjh.v6.i8.538. PMC 4163737. PMID 25232447.
- ↑ Knoblauch, Hans; Tennstedt, Cornelia; Brueck, Wolfgang; Hammer, Hannes; Vulliamy, Tom; Dokal, Inderjeet; Lehmann, Rüdiger; Hanefeld, Folker; Tinschert, Sigrid (2003). "Two brothers with findings resembling congenital intrauterine infection-like syndrome (pseudo-TORCH syndrome)". American Journal of Medical Genetics. 120A (2): 261–265. doi:10.1002/ajmg.a.20138. ISSN 0148-7299. PMID 12833411.
- ↑ Vivarelli, Rossella; Grosso, Salvatore; Cioni, Maddalena; Galluzzi, Paolo; Monti, Lucia; Morgese, Guido; Balestri, Paolo (March 2001). "Pseudo-TORCH syndrome or Baraitser–Reardon syndrome: diagnostic criteria". Brain and Development. 23 (1): 18–23. doi:10.1016/S0387-7604(00)00188-1. ISSN 0387-7604. PMID 11226724.
- ↑ Stewart, Andrew D.; Logsdon, John M.; Kelley, Steven E. (April 2005). "An empirical study of the evolution of virulence under both horizontal and vertical transmission". Evolution. 59 (4): 730–739. doi:10.1554/03-330. ISSN 0014-3820. PMID 15926685.
- ↑ Joo, Esther; Carmack, Anne; Garcia-Buñuel, Elizabeth; Kelly, Chester J. (February 2000). "Implementation of guidelines for HIV counseling and voluntary HIV testing of pregnant women". American Journal of Public Health. 90 (2): 273–276. doi:10.2105/AJPH.90.2.273. ISSN 0090-0036. PMC 1446152. PMID 10667191.
- ↑ Cavalli-Sforza, Luigi Luca; Feldman, Marcus W. (1981). Cultural Transmission and Evolution: A Quantitative Approach. Monographs in Population Biology. 16. Princeton University Press. ISBN 0-691-08283-9. Retrieved 30 April 2016.
- ↑ Syal K and Karande AA. IgG2 Subclass Isotype Antibody and Intrauterine Infections. Current Science Vol. 102, No. 11, 10 June 2012.