Second-degree atrioventricular block
| Second-degree atrioventricular block | |
|---|---|
 | |
| Classification and external resources | |
| Specialty | Cardiology |
| ICD-10 | I44.1 |
| ICD-9-CM | 426.12, 426.13 |
| DiseasesDB | 10477 |
| eMedicine | emerg/234 |
Second-degree atrioventricular block (AV block) is a disease of the electrical conduction system of the heart. It is a conduction block between the atria and ventricles.
The presence of second-degree AV block is diagnosed when one or more (but not all) of the atrial impulses fail to conduct to the ventricles due to impaired conduction.
Signs and symptoms
Most people with Wenckebach (Type I Mobitz) do not show symptoms. However, those that do usually display one or more of the following:
- Light-headedness
- Dizziness
- Syncope (fainting)
Types
There are two non-distinct types of second-degree AV block, called Type 1 and Type 2. In both types, a P wave is blocked from initiating a QRS complex; but, in Type 1, there are increasing delays in each cycle before the omission, whereas, in Type 2, there is no such pattern.[1]
Type 1 second-degree heart block is considered a more benign entity than type 2 second-degree heart block.[2]
Both types are named after Woldemar Mobitz.[3][4] Type I is also named for Karel Frederik Wenckebach,[5] and type II is also named for John Hay.[6][7]
Type 1 (Mobitz I/Wenckebach)
Type 1 Second-degree AV block, also known as Mobitz I or Wenckebach periodicity, is almost always a disease of the AV node.
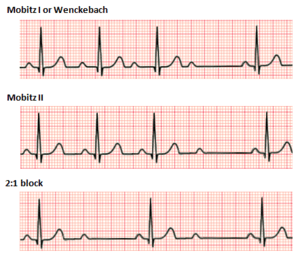
Mobitz I heart block is characterized by progressive prolongation of the PR interval on the electrocardiogram (ECG) on consecutive beats followed by a blocked P wave (i.e., a 'dropped' QRS complex). After the dropped QRS complex, the PR interval resets and the cycle repeats.
One of the baseline assumptions when determining if an individual has Mobitz I heart block is that the atrial rhythm has to be regular. If the atrial rhythm is not regular, there could be alternative explanations as to why certain P waves do not conduct to the ventricles.
This is almost always a benign condition for which no specific treatment is needed. In symptomatic cases, intravenous atropine or isoproterenol may transiently improve conduction.[8]

Type 2 (Mobitz II/Hay)
Type 2 Second-degree AV block, also known as "Mobitz II," is almost always a disease of the distal conduction system (His-Purkinje System).
Mobitz II heart block is characterized on a surface ECG by intermittently nonconducted P waves not preceded by PR prolongation and not followed by PR shortening. There is usually a fixed number of non-conducted P waves for every successfully conducted QRS complex, and this ratio is often specified in describing Mobitz II blocks. For example, Mobitz II block in which there are two P waves for every one QRS complex may be referred to as "2:1 Mobitz II block".[9]:181
The medical significance of this type of AV block is that it may progress rapidly to complete heart block, in which no escape rhythm may emerge. In this case, the person may experience a Stokes-Adams attack, cardiac arrest, or sudden cardiac death. The definitive treatment for this form of AV Block is an implanted pacemaker.
The impairment is usually below the AV node.[10] Although the terms infranodal block or infrahisian block are often applied to this disorder, they refer to the anatomic location of the block, whereas Mobitz II refers to an electrocardiographic pattern.
P:QRS Ratios
Because type I Mobitz block occurs in regular cycles, there is always a fixed ratio between the number of P waves and the number of QRS complexes per cycle. This ratio is often specified when describing the block. For example, a Mobitz type I block which has 4 P waves and 3 QRS complexes per cycle may be referred to as "4:3 Mobitz Type I block".[9]:179
Type II Mobitz block also usually occurs with a fixed P:QRS ratio, with a set number of P waves for every successfully elicited QRS.[9]:179 This ratio is also frequently specified in referring to "3:1", "4:1", "5:1", or higher Mobitz type II block. Higher numbers of P waves for every QRS indicate more severe block.[9]:181 Of course, because type II Mobitz block is unstable by nature, it is common for the P:QRS ratio in Mobitz type II block to change over time.
The P:QRS ratio is always of the form "X:(X-1)" in type I Mobitz block and of the form "X:1" in type 2 Mobitz block because of the nature of the pattern of each. Thus one may leave out the type and refer to "3:1 Mobitz block" or "4:3 Mobitz block", for example, without creating ambiguity, except in the case of 2:1 block.
2:1 AV Block
In the case of 2:1 block (2 P waves for every QRS complex) it is impossible to differentiate type I from type II Mobitz block based solely on the P:QRS ratio or on a pattern of lengthening PR intervals.[9]:182 In this case, a lengthened PR interval with a normal QRS width is most likely indicative of a type I-like pathology, and a normal PR interval with a widened QRS is most likely indicative of a type II-like pathology.[9]:182
See also
- Electrocardiogram (ECG or EKG)
- SA node
- AV node
- Atrioventricular block
- First-degree AV block
- Third-degree AV block
References
- ↑ "Lesson VI - ECG Conduction Abnormalities". Retrieved 2009-01-07.
- ↑ http://health.medicscientist.com/wp-content/uploads/2011/04/SeconddegreeAVblock2_thumb.jpg
- ↑ synd/2824 at Who Named It?
- ↑ W. Mobitz. Über die unvollständige Störung der Erregungsüberleitung zwischen Vorhof und Kammer des menschlichen Herzens. Zeitschrift für die Gesamte Experimentelle Medizin, Berlin 1924, 41: 180–237.
- ↑ K. F. Wenckebach. De Analyse van den onregelmatigen Pols. III. Over eenige Vormen van Allorythmie en Bradykardie. Nederlandsch Tijdschrift voor Geneeskunde, Amsterdam, 1898, 2: 1132.
- ↑ Silverman ME, Upshaw CB, Lange HW (August 2004). "Woldemar Mobitz and His 1924 classification of second-degree atrioventricular block". Circulation. 110 (9): 1162–7. doi:10.1161/01.CIR.0000140669.35049.34. PMID 15339865.
- ↑ J. Hay. Bradycardia and cardiac arrhythmia produced by depression of certain of the functions of the heart. The Lancet 1906, 1: 139–143.
- ↑ Lilly, L. S., Pathophysiology of Heart Disease. Baltimore: Lippincott Williams & Wilkins; 2007
- 1 2 3 4 5 6 Dubin, Dale (2000). Rapid interpretation of EKG's : ... an interactive course (6. ed.). Tampa, Fla.: Cover Publ. ISBN 978-0912912066.
- ↑ Wogan JM, Lowenstein SR, Gordon GS (1993). "Second-degree atrioventricular block: Mobitz type II". J Emerg Med. 11 (1): 47–54. doi:10.1016/0736-4679(93)90009-V. PMID 8445186.
{kind=link}