Peripherally inserted central catheter


A peripherally inserted central catheter (PICC or PIC line), less commonly called a percutaneous indwelling central catheter, is a form of intravenous access that can be used for a prolonged period of time (e.g., for long chemotherapy regimens, extended antibiotic therapy, or total parenteral nutrition) or for administration of substances that should not be done peripherally (e.g., antihypotensive agents aka pressors). It is a catheter that enters the body through the skin (percutaneously) at a peripheral site, extends to the superior vena cava (a central venous trunk), and stays in place (dwells within the veins) for days or weeks.
First described in 1975,[1] it is an alternative to central venous catheters such as subclavian lines, internal jugular lines or femoral lines, which have higher rates of infection—subclavian and jugular line placements may result in pneumothorax (air in the pleural space of lung), while PICC lines have no such issue because of the method of placement.
Medical uses
In those who are very unwell PICC lines are appropriate when more than two weeks of treatment is needed.[2]
Side effects
Side effects include blood clots and infection.[2]
Other complications may include catheter occlusion, phlebitis and bleeding. Urokinase or low-dose tPA may be used to break down obstructions. The type of occlusion (caused by medication precipitate or by thrombus) may determine which drug will be used in an attempt to clear the line. To decrease the risk of infection, particularly a blood stream infection, those involved in the management of the PICC must adhere to strict infection control procedures.[3]
Insertion
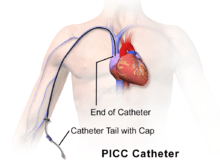
A PICC is inserted in a peripheral vein in the arm, such as the cephalic vein, basilic vein or brachial vein, and then advanced proximally toward the heart through increasingly larger veins, until the tip rests in the distal superior vena cava or cavoatrial junction.
PICCs are usually inserted by physicians, physician assistants (in the US), radiologist assistants (in the US), respiratory therapists, nurse practitioners, or specially trained certified registered nurses and radiologic technologists using ultrasound, chest radiographs, and fluoroscopy to aid in their insertion and to confirm placement. PICC insertion is a sterile procedure, but does not require the use of an operating room. When done at bedside (that is, in the patient's room), a suitable sterile field must be established and maintained throughout the procedure. For this reason, visitors are normally requested to leave the room until the insertion is complete, and some form of skin preparation should be used to clean the patient's skin.
The insertable portion of a PICC varies from 25 to 60 cm in length, that being adequate to reach the desired tip position in most patients. Some lines are designed to be trimmed to the desired length before insertion; others are simply inserted to the needed depth with the excess left outside. As supplied, the line has a guide wire inside. This wire is provided to stiffen the (otherwise very flexible) line so it can be threaded through the veins. The wire is removed and discarded after insertion.
The PICC is also provided with a "wing" having holes for either sutures or an adhesive securing device. Securing the catheter prevents post-insertion movements of the line, which otherwise could place the tip in an unsafe position.
Usage
PICCs can remain in situ for extended periods of time, from seven days to 12 months, although little information is available with respect to viability timeframes. They are used in both the hospital and community settings. PICCs can be used for intravenous delivery of total parenteral nutrition (TPN), chemotherapy, antibiotics or other medications, and can also be used for blood sampling if the lumen is 4 French or larger in size (Arrow and Bard manufacturers guidelines). To maintain patency, PICC management should include regular flushing with normal saline and "locking" with Heparin or normal saline when not in use. The type of locking procedure depends on the type of PICC and bung; Groshong PICCs have a three-way valve at the tip so the use of a heparin lock is not necessary, and there are no clamps on the external length. In comparison, Arrow PICCs have clamps on the exterior line and require a heparin lock. The use of heparin to maintain line patency, though, is questionable, and currently randomized clinical control trials are investigating this further. Heparin locks have been associated with complications, including heparin-induced thrombocytopaenia.[4]
Blood pressure should not be taken on the arm with a PICC,[5] which is a problem if there are reasons not to take pressure on the other arm, such as a dialysis shunt, absence, cast, infection, lymph node removal, etc. Blood pressure readings on legs are often 10–20% higher than those on the brachial artery.[6]
Certain types of PICCs have recently been approved by the FDA for use in power injection. These types, often referred to as power-injectable PICCs, are designed to withstand the high pressures associated with radiocontrast studies.
PICCs can also be used to measure central venous pressure, which is a rough estimate of the right atrial pressures of the heart and can give valuable information about fluid status.
Removal
In most cases, removal of a PICC is a simple procedure. Generally, the catheter line can be safely and quickly removed by a trained nurse, even in the patient's own home, in a matter of minutes. After removal, the insertion site is normally bandaged with sterile gauze and kept dry for a few days, during which the wound can close and begin healing. Usually, a smaller adhesive bandage can be placed over the wound site after the gauze is removed if the wound is slow to heal. Tip of the catheter is sent for MCS ( microscopy culture and sensitivity)if the patient is systemically unwell at the time of removal of the PICC. In certain units, it is sent as routine investigation.
See also
References
- ↑ Hoshal VL (May 1975). "Total intravenous nutrition with peripherally inserted silicone elastomer central venous catheters". Arch Surg. 110 (5): 644–6. doi:10.1001/archsurg.1975.01360110190032. PMID 805577.
- 1 2 Chopra, V; Flanders, SA; Saint, S; Woller, SC; O'Grady, NP; Safdar, N; Trerotola, SO; Saran, R; Moureau, N; Wiseman, S; Pittiruti, M; Akl, EA; Lee, AY; Courey, A; Swaminathan, L; LeDonne, J; Becker, C; Krein, SL; Bernstein, SJ (15 September 2015). "The Michigan Appropriateness Guide for Intravenous Catheters (MAGIC): Results From a Multispecialty Panel Using the RAND/UCLA Appropriateness Method.". Annals of Internal Medicine. 163 (6 Suppl): S1–S40. doi:10.7326/M15-0744. PMID 26369828.
- ↑ Guidelines for the Prenention of Intravascular Catheter-Related Infections, Centre for Disease Control 2011; Infusion Nurses Standards, 2010).Centre for Disease Control
- ↑
- ↑ U Wisconsin, Preparing and Caring, accessed July 24, 2013
- ↑ Measuring Blood Pressure in Legs, by Erica Brownfield, MD, accessed July 24, 2013
Further reading
- Bender, C. M., Rosenzweig, M., & Green, E. (2006). "Cancer". In S. Goldsworthy & M. A. Barry. Medical-Surgical Nursing in Canada: Assessment and Management of Clinical Problems (1st Canadian ed.). Mosby: Toronto. ISBN 0-7796-9969-6.