Occipital horn syndrome
| Occipital horn syndrome | |
|---|---|
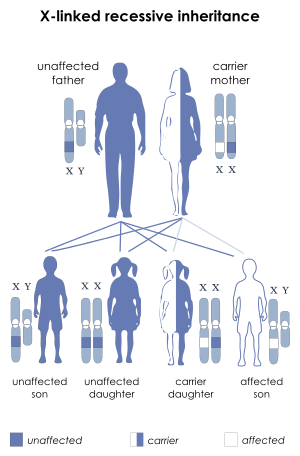 | |
| X-linked recessive | |
| Classification and external resources | |
| Specialty | endocrinology |
| ICD-10 | E83.0 |
| OMIM | 304150 |
| DiseasesDB | 33413 |
Occipital horn syndrome (OHS), formerly considered a variant of Ehlers-Danlos syndrome,[1] is an X-linked recessive connective tissue disorder. It is caused by a deficiency in the transport of the essential mineral copper, associated with mutations in the ATP7A gene.[2][3] Only about 2/3 of children with OHS are thought to have genetically inherited the disorder; the other 1/3 do not have the disease in their family history. Since the disorder is X-linked recessive the disease affects more males. This is because they do not have a second X chromosome, unlike females, so essentially are lacking the 'backup' copy with proper function. Females are much more likely to be carriers only. For a female to be affected they must carry two defective X chromosomes, not just one.[4] The disorder is considered a milder variant of Menkes disease.[5]
Signs/symptoms
It is characterized by a deficiency in biliary copper excretion that causes deformations in the skeleton. These include projections on the back of the skull (parasagittal bone exostoses arising from the occipital bone—the so-called "occipital horns") as well as deformities of the elbow, radial head dislocation, hammer-shaped lateral ends of the clavicles, and abnormalities of the hips and pelvis.[1] OHS presents in early to middle childhood.[4] Children may present with features such as:
- Normal/slightly delayed intelligence
- Long neck, high arched palate, long face, high forehead
- Looseness of skin and "double jointed"
- Inguinal Hernias
- Twisting of blood vessels
- Bladder diverticula
- Dysautonomia—inability to regulate parts of the nervous system
- Chronic Diarrhea
- Coarse hair
Treatment
Courses of treatment for children with is dependent upon the severity of their case. Children with OHS often receive physical and occupational therapy.[4] They may require a feeding tube to supplement nourishment if they are not growing enough. In an attempt to improve the neurological condition (seizures) copper histidine or copper chloride injections can be given early in the child’s life. However, copper histidine injections have been shown ineffective in studies of copper metabolic-connective tissue disorders such as OHS.[6]
See also
References
- 1 2 Online Mendelian Inheritance in Man (OMIM) 304150
- ↑ Scheiber, Ivo; Dringen, Ralf; Mercer, Julian F. B. (2013). "Chapter 11. Copper: Effects of Deficiency and Overload". In Astrid Sigel, Helmut Sigel and Roland K. O. Sigel. Interrelations between Essential Metal Ions and Human Diseases. Metal Ions in Life Sciences. 13. Springer. pp. 359–387. doi:10.1007/978-94-007-7500-8_11.
- ↑ Tang J, Robertson S, Lem KE, Godwin SC, Kaler SG (November 2006). "Functional copper transport explains neurologic sparing in occipital horn syndrome". Genet. Med. 8 (11): 711–8. doi:10.1097/01.gim.0000245578.94312.1e. PMID 17108763.
- 1 2 3 Horn Syndrome, 9 August 2004.
- ↑ Kennerson ML, Nicholson GA, Kaler SG, et al. (March 2010). "Missense mutations in the copper transporter gene ATP7A cause X-linked distal hereditary motor neuropathy". Am. J. Hum. Genet. 86 (3): 343–52. doi:10.1016/j.ajhg.2010.01.027. PMC 2833394
 . PMID 20170900.
. PMID 20170900. - ↑ Kodama, H.; C. Fujisima, W. Bhadhprasit. (November 2010). "Pathology, clinical features and treatments of congenital copper metabolic disorders - Focus on neurologic aspects.". Brain & Development.
External links
- GeneReviews/NCBI/NIH/UW entry on ATP7A-Related Copper Transport Disorders
- Occipital horn syndrome at NIH's Office of Rare Diseases