Nerve conduction study

A nerve conduction study (NCS) is a medical diagnostic test commonly used to evaluate the function, especially the ability of electrical conduction, of the motor and sensory nerves of the human body. These tests may be performed by medical specialists such as clinical neurophysiologists, chiropractors, physiatrists (physical medicine and rehabilitation [PMR] physicians), and neurologists who subspecialize in electrodiagnostic medicine. In the United States, neurologists and physiatrists receive training in electrodiagnostic medicine (performing needle electromyography and NCSs) as part of residency training and in some cases acquire additional expertise during a fellowship in clinical neurophysiology, electrodiagnostic medicine, or neuromuscular medicine.[1][2][3] Outside the US, clinical neurophysiologists learn needle EMG and NCS testing.
Nerve conduction velocity (NCV) is a common measurement made during this test. The term NCV often is used to mean the actual test, but this may be misleading, since velocity is only one measurement in the test suite.
Medical uses
Nerve conduction studies along with needle electromyography measure nerve and muscle function, and may be indicated when there is pain in the limbs, weakness from spinal nerve compression, or concern about some other neurologic injury or disorder.[4] Spinal nerve injury does not cause neck, mid back pain or low back pain, and for this reason, evidence has not shown EMG or NCS to be helpful in diagnosing causes of axial lumbar pain, thoracic pain, or cervical spine pain.[4]
Nerve conduction studies are used mainly for evaluation of paresthesias (numbness, tingling, burning) and/or weakness of the arms and legs. The type of study required is dependent in part by the symptoms presented. A physical exam and thorough history also help to direct the investigation. Some of the common disorders that can be diagnosed by nerve conduction studies are:
- Carpal tunnel syndrome
- Cubital Tunnel Syndrome
- Guillain–Barré syndrome
- Guyon's canal syndrome
- Peripheral neuropathy
- Peroneal neuropathy
- Spinal disc herniation
- Tarsal Tunnel Syndrome
- Ulnar neuropathy
Technique
The nerve conduction study consists of the following components
The nerve conduction study is often combined with needle electromyography. The Department of Health and Human Services Inspector General recently identified the use of NCSs without a needle electromyography at the same time a sign of questionable billing.[5]
Motor NCS
Motor NCS are performed by electrical stimulation of a peripheral nerve and recording from a muscle supplied by this nerve. The time it takes for the electrical impulse to travel from the stimulation to the recording site is measured. This value is called the latency and is measured in milliseconds (ms). The size of the response - called the amplitude - is also measured. Motor amplitudes are measured in millivolts (mV). By stimulating in two or more different locations along the same nerve, the NCV across different segments can be determined. Calculations are performed using the distance between the different stimulating electrodes and the difference in latencies.
Sensory NCS
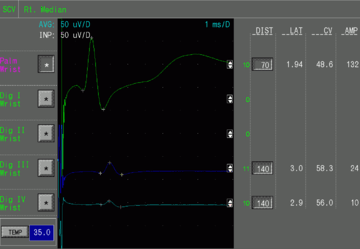
Sensory NCS are performed by electrical stimulation of a peripheral nerve and recording from a purely sensory portion of the nerve, such as on a finger. Like the motor studies, sensory latencies are on the scale of milliseconds. Sensory amplitudes are much smaller than the motor amplitudes, usually in the microvolt (μV) range. The sensory NCV is calculated based upon the latency and the distance between the stimulating and recording electrodes.
F-wave study
F-wave study uses supramaximal stimulation of a motor nerve and recording of action potentials from a muscle supplied by the nerve. This is not a reflex, per se, in that the action potential travels from the site of the stimulating electrode in the limb to the spinal cord's ventral horn and back to the limb in the same nerve that was stimulated. The F-wave latency can be used to derive the conduction velocity of nerve between the limb and spine, whereas the motor and sensory nerve conduction studies evaluate conduction in the segment of the limb. F waves vary in latency and an abnormal variance is called "chrono dispersion". Conduction velocity is derived by measuring the limb length, D, in millimeters from the stimulation site to the corresponding spinal segment (C7 spinous process to wrist crease for median nerve). This is multiplied by 2 as it goes to the cord and returns to the muscle (2D). 2D is divided by the latency difference between mean F and M and 1 millisecond subtracted (F-M-1). The formula is .

H-reflex study
H-reflex study uses stimulation of a nerve and recording the reflex electrical discharge from a muscle in the limb. This also evaluates conduction between the limb and the spinal cord, but in this case, the afferent impulses (those going toward the spinal cord) are in sensory nerves while the efferent impulses (those coming from the spinal cord) are in motor nerves. This process cannot be changed.
Specialized testing
Repetitive nerve stimulation
Small-pain-fibers method
In 1998, a small-pain-fibers (spf-NCS) method was cleared by the FDA. This method uses an electrical stimulus with a neuroselective frequency to determine the minimum voltage causing conduction. Rather than comparing the data with population averages on a bell-shape curve, which at best has about 65% sensitivity, the patient is his own control. In a three-year LSU Pain Center study, it was found that the nerve requiring the greatest voltage to cause conduction of the A-delta (Fast Pain) fibers identified nerve root pathology with 95% sensitivity. Besides being painless, the test is fast. This test can determine nerve impingement/pathology (pain causing) within the spine (nerve root level) where EMG and Velocity Tests fail. The test uses a potentiometer to objectively measure the amplitude of the action potential at a distant site along the nerve being tested. The patient confirms a sensation when the nerve fires. Objectivity of the patient's response is confirmed by the measurement of nerve recruitment for surrounding nerves and is displayed on the instrument. The impinged nerve (pain fibers) can only report (peak) momentarily while recruiting other nerves to assist and sustain the reporting of the stimulus. Non impinged nerves (pain fibers) do not recruit surrounding nerves and this is readily seen on the display.
The spf-NCS does not require myelin loss to detect function change, so velocity is not measured. The Small-Pain-Fibers NCS (pf-NCS) is the preferred test with over 95% accuracy for determining the spine level(s) and side(s) for Small Pain Fiber impingement/pathology allowing for the most accurate diagnosis and treatment procedures for patients experiencing back pain. Patients diagnosed with the EMG/NCV studies alone (while experiencing pain but having no significant myelin loss) were misdiagnosed in over 50% of cases including the diagnosis and treatment of incorrect nerve root levels and sides in patients.
Interpretation of nerve conductions
The interpretation of nerve conduction studies is complex and requires the expertise of medical practitioners such as clinical neurophysiologists, neurologists or physiatrists. In general, different pathological processes result in changes in latencies, motor, and/or sensory amplitudes, or slowing of the conduction velocities to differing degrees. For example, slowing of the NCV usually indicates there is damage to the myelin. Another example, slowing across the wrist for the motor and sensory latencies of the median nerve indicates focal compression of the median nerve at the wrist, called carpal tunnel syndrome. On the other hand, slowing of all nerve conductions in more than one limb indicates generalized diseased nerves, or generalized peripheral neuropathy. People with diabetes mellitus often develop generalized peripheral neuropathy.
Patient risk
Nerve conduction studies are very helpful to diagnose certain diseases of the nerves of the body. The test is not invasive, but can be painful due to the electrical shocks. The shocks are associated with a low amount of electric current so they are not dangerous to anyone. Patients with a permanent pacemaker or other such implanted stimulators such as deep brain stimulators or spinal cord stimulators must tell the examiner prior to the study. This does not prevent the study, but special precautions are taken.
Cardiac pacemakers and implanted cardiac defibrillators (ICDs) are used increasingly in clinical practice, and no evidence exists indicating that performing routine electrodiagnostic studies on patients with these devices pose a safety hazard. However, there are theoretical concerns that electrical impulses of nerve conduction studies (NCS) could be erroneously sensed by devices and result in unintended inhibition or triggering of output or reprogramming of the device. In general, the closer the stimulation site is to the pacemaker and pacing leads, the greater the chance for inducing a voltage of sufficient amplitude to inhibit the pacemaker. Despite such concerns, no immediate or delayed adverse effects have been reported with routine NCS.[6]
No known contraindications exist from performing needle EMG or NCS on pregnant patients. In addition, no complications from these procedures have been reported in the literature. Evoked potential testing, likewise, has not been reported to cause any problems when it is performed during pregnancy.[6]
See also
References
- ↑ http://www.acgme.org/acgmeweb/Portals/0/PFAssets/ProgramRequirements/183-343_neuromuscular_med_07012014_1-YR.pdf
- ↑ http://www.acgme.org/acgmeweb/Portals/0/PFAssets/ProgramRequirements/187_clinical_neurophysiology_07012014_1-YR.pdf
- ↑ http://www.acgme.org/acgmeweb/Portals/0/PFAssets/ProgramRequirements/340_physical_medicine_rehabilitation_07012014.pdf
- 1 2 North American Spine Society (February 2013), "Five Things Physicians and Patients Should Question", Choosing Wisely: an initiative of the ABIM Foundation, North American Spine Society, retrieved 25 March 2013, which cites
- Sandoval, AE (Nov 2010). "Electrodiagnostics for low back pain.". Physical Medicine and Rehabilitation Clinics of North America. 21 (4): 767–76. doi:10.1016/j.pmr.2010.06.007. PMID 20977959.
- North American Spine Society (2011). "Diagnosis and treatment of degenerative lumbar spinal stenosis". Burr Ridge, Illinois: Agency for Healthcare Research and Quality: 104.
- ↑ http://oig.hhs.gov/oei/reports/oei-04-12-00420.pdf
- 1 2 http://www.aanem.org/getmedia/2034191e-583b-4c55-b725-fc38ea8262e2/risksinEDX.pdf.aspx.
External links
- EMG & Nerve Conduction Education & Resources
- Association of EMG technologists of Canada
- American Association of Neuromuscular & Electrodiagnostic Medicine
- American Board of Electrodiagnostic Medicine
- Details of NCV from National Institutes of Health
- WebMD summary of EMG and NCS