Metformin
 | |
 | |
| Clinical data | |
|---|---|
| Pronunciation | /mɛtˈfɔːrmᵻn/, met-FAWR-min |
| Trade names | Glucophage, other |
| AHFS/Drugs.com | Monograph |
| MedlinePlus | a696005 |
| License data | |
| Pregnancy category | |
| Routes of administration | oral |
| ATC code | A10BA02 (WHO) |
| Legal status | |
| Legal status | |
| Pharmacokinetic data | |
| Bioavailability | 50–60%[1][2] |
| Protein binding | Minimal[1] |
| Metabolism | Not by liver[1] |
| Biological half-life | 4-8.7 hours[1] |
| Excretion | Urine (90%)[1] |
| Identifiers | |
| |
| CAS Number |
657-24-9 |
| PubChem (CID) | 4091 |
| IUPHAR/BPS | 4779 |
| DrugBank | DB00331 |
| ChemSpider |
3949 |
| UNII |
9100L32L2N hydrochloride: 786Z46389E |
| KEGG |
D04966 |
| ChEBI |
CHEBI:6801 |
| ChEMBL |
CHEMBL1431 |
| Chemical and physical data | |
| Formula | C4H11N5 |
| Molar mass | 129.16364 g/mol |
| 3D model (Jmol) | Interactive image |
| |
| |
Metformin, marketed under the tradename Glucophage among others, is the first-line medication for the treatment of type 2 diabetes.[3][4] This is particularly true in people who are overweight.[5] It is also used in the treatment of polycystic ovary syndrome.[3] Limited evidence suggests metformin may prevent the cardiovascular disease and cancer complications of diabetes.[6][7] It is not associated with weight gain.[7] It is taken by mouth.[3]
Metformin is generally well tolerated.[8] Common side effects include diarrhea, nausea, and abdominal pain.[3] It has a low risk of developing low blood sugar.[3] High blood lactic acid level is a concern if the drug is prescribed inappropriately and in overdose.[9] It should not be used in those with liver disease or kidney problems.[3] While there is no clear harm if used during pregnancy, insulin is generally preferred for gestational diabetes.[3][10] Metformin is in the biguanide class.[3] It works by decreasing glucose production by the liver and increasing the insulin sensitivity of body tissues.[3]
Metformin was discovered in 1922.[11] Study in humans began in 1950s by French physician Jean Sterne.[11] It was introduced as a medication in France in 1957 and the United States in 1995.[3][12] It is on the World Health Organization's List of Essential Medicines, the most important medications needed in a basic healthcare system.[13] Metformin is believed to be the most widely used medication for diabetes which is taken by mouth.[11] It is available as a generic medication.[3] The wholesale price in the developed world is between 0.21 and 5.55 USD per month as of 2014.[14] In the United States, it costs 5 to 25 USD per month.[3]
Medical uses
Metformin is primarily used for type 2 diabetes, but is increasingly being used in polycystic ovary syndrome.[3][15]
Type 2 diabetes
The American Diabetes Association] recommends metformin as a first-line agent to treat type 2 diabetes.[16][17]
Efficacy
The UK Prospective Diabetes Study, a large clinical trial performed in 1980-90s, provided evidence that metformin reduced the rate of adverse cardiovascular outcomes in overweight patients with type 2 diabetes relative to other antihyperglycemic agents.[18] However, accumulated evidence from other and more recent trials has reduced confidence in the efficacy of metformin for cardiovascular disease prevention.[19][20] Treatment guidelines for major professional associations including the European Association for the Study of Diabetes, the European Society for Cardiology, and the American Diabetes Association, now describe evidence for the cardiovascular benefits of metformin as equivocal.[17][21] According to the American College of Physicians in 2012, low-quality evidence indicates metformin monotherapy is associated with lower cardiovascular mortality than sulfonylurea monotherapy and metformin monotherapy is associated with fewer cardiovascular events than metformin-sulfonylurea combination therapy. Evidence for other comparisons is described as unclear.[22] A 2014 review found tentative evidence that people treated with sulfonylureas have fewer non-fatal cardiovascular events than those treated with metformin (RR 0.67) but a higher risk of severe low blood sugar events (RR 5.64). There was not enough data available to determine the relative risk of death or of death from heart disease.[23]
Metformin has little or no effect on body weight compared with placebo in type 2 diabetes,[24] although it causes weight loss compared with sulfonylureas, since sulfonylureas are associated with weight gain.[24] There is some limited evidence that metformin may be associated with weight loss in obesity in the absence of diabetes.[25][26] Metformin has a lower risk of hypoglycemia than the sulfonylureas,[27][28] although hypoglycemia has uncommonly occurred during intense exercise, calorie deficit, or when used with other agents to lower blood glucose.[29][30] Metformin modestly reduces LDL and triglyceride levels.[27][28]
Prediabetes
Metformin treatment of people at risk for type 2 diabetes may decrease their chances of developing the disease, although intensive physical exercise and dieting work significantly better for this purpose. In a large U.S. study known as the Diabetes Prevention Program, participants were divided into groups and given either placebo, metformin, or lifestyle intervention, and followed for an average of three years. The intensive program of lifestyle modifications included a 16-lesson training on dieting and exercise followed by monthly individualized sessions with the goals to decrease the body weight by 7% and engage in a physical activity for at least 150 minutes per week. The incidence of diabetes was 58% lower in the lifestyle group and 31% lower in individuals given metformin. Among younger people with a higher body mass index, lifestyle modification was no more effective than metformin, and for older individuals with a lower body mass index, metformin was no better than placebo in preventing diabetes.[31] After ten years, the incidence of diabetes was 34% lower in the group of participants given diet and exercise and 18% lower in those given metformin.[32] It is unclear whether metformin slowed down the progression of prediabetes to diabetes (true preventive effect), or the decrease of diabetes in the treated population was simply due to its glucose-lowering action (treatment effect).[33]
Polycystic ovary syndrome
Antidiabetic therapy has been proposed as a treatment for polycystic ovary syndrome (PCOS), a condition frequently associated with insulin resistance, since the late 1980s.[34] The use of metformin in PCOS was first reported in 1994, in a small study conducted at the University of the Andes, Venezuela.[35][36] The United Kingdom's National Institute for Health and Clinical Excellence recommended in 2004 that women with PCOS and a body mass index above 25 be given metformin for anovulation and infertility when other therapies have failed to produce results.[37] However, two clinical studies completed in 2006–2007 returned mostly negative results, with metformin being no better than placebo, and a metformin-clomifene combination no better than clomifene alone.[38][39] Reflecting this, subsequent reviews noted large randomized controlled trials have, in general, not shown the promise suggested by the early small studies. UK and international clinical practice guidelines do not recommend metformin as a first-line treatment[40] or do not recommend it at all, except for women with glucose intolerance.[41] The guidelines suggest clomiphene as the first medication option and emphasize lifestyle modification independently from the drug treatment.
In a dissenting opinion, a systematic review of four head-to-head comparative trials of metformin and clomifene found them equally effective for infertility.[42] Four positive studies of metformin were in women not responding to clomifene, while the population in the negative studies was drug-naive or uncontrolled for the previous treatment. Metformin should be used as a second-line drug if clomifene treatment fails.[43] Another review recommended metformin unreservedly as a first-line treatment option because it has positive effects not only on anovulation, but also on insulin resistance, hirsutism, and obesity often associated with PCOS.[44] A Cochrane Collaboration review found metformin improves ovulation and pregnancy rates, particularly when combined with clomifene, but is not associated with any increase in the number of live births.[45]
The use of metformin during all parts of pregnancy is controversial.[46] One review found that when taken during pregnancy it reduces the number of complications during pregnancy and does not appear to cause developmental delays.[47]
Gestational diabetes
Several observational studies and randomized, controlled trials have found metformin to be as effective and safe as insulin for the management of gestational diabetes.[48][49] Nonetheless, several concerns have been raised regarding studies published thus far, and evidence on the long-term safety of metformin for both mother and child is still lacking.[50]
Metformin is safe in pregnancy and women with gestational diabetes treated with metformin have less weight gain during pregnancy than those treated with insulin. Babies born to women treated with metformin have been found to develop less visceral fat, making them less prone to insulin resistance in later life.[51]
Contraindications
Metformin is contraindicated in people with any condition that could increase the risk of lactic acidosis, including kidney disorders (arbitrarily defined as creatinine levels over 150 μmol/l (1.7 mg/dl),[52]), lung disease and liver disease. According to the prescribing information, heart failure (in particular, unstable or acute congestive heart failure) increases the risk of lactic acidosis with metformin.[53] A 2007 systematic review of controlled trials, however, suggested metformin is the only antidiabetic drug not associated with any measurable harm in people with heart failure, and it may reduce mortality in comparison with other antidiabetic agents.[54]
Metformin is recommended to be temporarily discontinued before any radiographic study involving iodinated contrast agents, (such as a contrast-enhanced CT scan or angiogram), as the contrast dye may temporarily impair kidney function, indirectly leading to lactic acidosis by causing retention of metformin in the body.[55][56] Metformin can be resumed after two days, assuming kidney function is normal.[55][56]
Adverse effects
The most common adverse effect of metformin is gastrointestinal irritation, including diarrhea, cramps, nausea, vomiting, and increased flatulence; metformin is more commonly associated with gastrointestinal side effects than most other antidiabetic drugs.[28] The most serious potential side effect of metformin use is lactic acidosis; this complication is very rare, and the vast majority of these cases seem to be related to comorbid conditions, such as impaired liver or kidney function, rather than to the metformin itself.[57]
Metformin has also been reported to decrease the blood levels of thyroid-stimulating hormone in people with hypothyroidism,[58] The clinical significance of this is still unknown.
Gastrointestinal
In a clinical trial of 286 subjects, 53.2% of the 141 given immediate-release metformin (as opposed to placebo) reported diarrhea, versus 11.7% for placebo, and 25.5% reported nausea/vomiting, versus 8.3% for those on placebo.[59]
Gastrointestinal upset can cause severe discomfort; it is most common when metformin is first administered, or when the dose is increased. The discomfort can often be avoided by beginning at a low dose (1.0 to 1.7 grams per day) and increasing the dose gradually.
Long-term use of metformin has been associated with increased homocysteine levels[60] and malabsorption of vitamin B12.[61][62] Higher doses and prolonged use are associated with increased incidence of vitamin B12 deficiency,[63] and some researchers recommend screening or prevention strategies.[64]
Lactic acidosis
The most serious potential adverse effect of biguanide use is lactic acidosis ("metformin-associated lactic acidosis" or MALA). Though the incidence for MALA has been measured at about nine per 100,000 person-years,[65] this is not different from the background incidence of lactic acidosis in the general population. A systematic review concluded no data exists to definitively link metformin to lactic acidosis.[66] Lactic acidosis can be fatal in some cases.
Phenformin, another biguanide, was withdrawn from the market because of an increased risk of lactic acidosis (rate of 40-64 per 100,000 patient-years).[65] However, metformin is safer than phenformin, and the risk of developing lactic acidosis is not increased by the medication as long as it is not prescribed to known high-risk groups.[66]
Lactate uptake by the liver is diminished with metformin administration because lactate is a substrate for hepatic gluconeogenesis, a process which metformin inhibits. In healthy individuals, this slight excess is simply cleared by other mechanisms (including uptake by the kidneys, when their function is unimpaired), and no significant elevation in blood levels of lactate occurs.[27] When impaired kidney function is present, however, clearance of metformin and lactate is reduced, leading to increased levels of both, and possibly causing a buildup of lactic acid. Because metformin decreases liver uptake of lactate, any condition that may precipitate lactic acidosis is a contraindication to its use. Common causes of increased lactic acid production include alcoholism (due to depletion of NAD+ stores), heart failure, and respiratory disease (due to inadequate oxygenation of tissues); the most common cause of impaired lactic acid excretion is kidney disease.[67]
Metformin has also been suggested to increase production of lactate in the large intestine; this could potentially contribute to lactic acidosis in those with risk factors.[68] However, the clinical significance of this is unknown, and the risk of metformin-associated lactic acidosis is most commonly attributed to decreased hepatic uptake rather than increased intestinal production.[27][67][69]
Overdose
A review of intentional and accidental metformin overdoses reported to poison control centers over a five-year period found serious adverse events were rare, though the elderly appeared to be at greater risk.[70] A similar study where cases were reported to Texas poison control centers between 2000 and 2006 found ingested doses of more than 5,000 mg were more likely to involve serious medical outcomes in adults.[71] Survival following intentional overdoses with up to 63,000 mg (63 g) of metformin have been reported in the medical literature.[72] Fatalities following overdose are rare, but do occur.[73][74][75] In healthy children, unintentional doses of less than 1,700 mg are unlikely to cause any significant toxic effects.[76]
The most common symptoms following overdose appear to include vomiting, diarrhea, abdominal pain, tachycardia, drowsiness, and, rarely, hypoglycemia or hyperglycemia.[71][74] The major potentially life-threatening complication of metformin overdose is lactic acidosis, which is due to lactate accumulation.[77][78] Treatment of metformin overdose is generally supportive, as no specific antidote is known. Lactic acidosis is initially treated with sodium bicarbonate, although high doses are not recommended, as this may increase intracellular acidosis.[75] Acidosis that does not respond to administration of sodium bicarbonate may require further management with standard hemodialysis or continuous venovenous hemofiltration. These treatments are recommended in severe overdoses.[79] In addition, due to metformin's low molecular weight and lack of plasma protein binding, these techniques also have the benefit of removing metformin from blood plasma, preventing further lactate overproduction.[79]
Metformin may be quantified in blood, plasma, or serum to monitor therapy, confirm a diagnosis of poisoning, or assist in a medicolegal death investigation. Blood or plasma metformin concentrations are usually in a range of 1–4 mg/l in persons receiving the drug therapeutically, 40–120 mg/l in victims of acute overdosage, and 80–200 mg/l in fatalities. Chromatographic techniques are commonly employed.[80][81]
Interactions
The H2-receptor antagonist cimetidine causes an increase in the plasma concentration of metformin, by reducing clearance of metformin by the kidneys;[82] both metformin and cimetidine are cleared from the body by tubular secretion, and both, particularly the cationic (positively charged) form of cimetidine, may compete for the same transport mechanism.[83] A small double-blind, randomized study found the antibiotic cephalexin to also increase metformin concentrations by a similar mechanism;[84] theoretically, other cationic medications may produce the same effect.[83]
Mechanism of action
The exact mechanism of metformin is incompletely understood. The drug's main effect is to decrease hepatic glucose production.[68] Metformin also increases insulin sensitivity, which increases peripheral glucose uptake.[85]
Metformin decreases high blood sugar primarily by suppressing glucose production by the liver (hepatic gluconeogenesis).[68] The "average" person with type 2 diabetes has three times the normal rate of gluconeogenesis; metformin treatment reduces this by over one-third.[86] The molecular mechanism of metformin is incompletely understood: inhibition of the mitochondrial respiratory chain (complex I), activation of AMP-activated protein kinase (AMPK), inhibition of glucagon-induced elevation of cyclic adenosine monophosphate (cAMP) with reduced activation of protein kinase A (PKA), inhibition of mitochondrial glycerophosphate dehydrogenase, and an effect on gut microbiota have been proposed as potential mechanisms.[87][88][89]
Activation of AMPK, an enzyme that plays an important role in insulin signaling, whole body energy balance, and the metabolism of glucose and fats,[90] was required for metformin's inhibitory effect on the production of glucose by liver cells.[91] Activation of AMPK was required for an increase in the expression of small heterodimer partner, which in turn inhibited the expression of the hepatic gluconeogenic genes Phosphoenolpyruvate carboxykinase and glucose 6-phosphatase.[92] Metformin is frequently used in research along with AICA ribonucleotide as an AMPK agonist. More recent studies using mouse models in which the genes for AMPKα1 and α2 catalytic subunits (Prkaa1/2) or LKB1, an upstream kinase of AMPK, had been knocked out in hepatocytes, have raised doubts over the obligatory role of AMPK, since the effect of metformin was not abolished by loss of AMPK function.[87] The mechanism by which biguanides increase the activity of AMPK remains uncertain; however, metformin increases the concentration of cytosolic adenosine monophosphate (AMP) (as opposed to a change in total AMP or total AMP/adenosine triphosphate).[93] Increased cellular AMP has also been proposed to explain the inhibition of glucagon-induced increase in cAMP and activation of PKA.[87] Metformin and other biguanides may antagonize the action of glucagon, thus reducing fasting glucose levels.[94] Metformin also induces a profound shift in the faecal microbial community profile in diabetic mice and this may contribute to its mode of action possibly through an effect on glucagon-like peptide-1 secretion.[88]
In addition to suppressing hepatic glucose production, metformin increases insulin sensitivity, enhances peripheral glucose uptake (by inducing the phosphorylation of GLUT4 enhancer factor), decreases insulin-induced suppression of fatty acid oxidation,[85] and decreases absorption of glucose from the gastrointestinal tract. Increased peripheral use of glucose may be due to improved insulin binding to insulin receptors.[95] The increase in insulin binding after metformin treatment has also been demonstrated in patients with NIDDM.[96]
AMPK probably also plays a role in increased insulin[clarification requested], as metformin administration increases AMPK activity in skeletal muscle.[97] AMPK is known to cause GLUT4 deployment to the plasma membrane, resulting in insulin-independent glucose uptake. Some metabolic actions of metformin do appear to occur by AMPK-independent mechanisms; the metabolic actions of metformin in the heart muscle can occur independent of changes in AMPK activity and may be mediated by p38 MAPK- and PKC-dependent mechanisms.[98]
Chemistry
The usual synthesis of metformin, originally described in 1922 and reproduced in multiple later patents and publications, involves the one-pot reaction of dimethylamine hydrochloride and 2-cyanoguanidine over heat.[99][100]
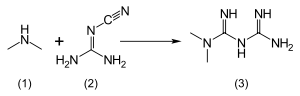
According to the procedure described in the 1975 Aron patent,[101] and the Pharmaceutical Manufacturing Encyclopedia,[102] equimolar amounts of dimethylamine and 2-cyanoguanidine are dissolved in toluene with cooling to make a concentrated solution, and an equimolar amount of hydrogen chloride is slowly added. The mixture begins to boil on its own, and after cooling, metformin hydrochloride precipitates with a 96% yield.
Pharmacokinetics
Metformin has an oral bioavailability of 50–60% under fasting conditions, and is absorbed slowly.[83][103] Peak plasma concentrations (Cmax) are reached within one to three hours of taking immediate-release metformin and four to eight hours with extended-release formulations.[83][103] The plasma protein binding of metformin is negligible, as reflected by its very high apparent volume of distribution (300–1000 l after a single dose). Steady state is usually reached in one or two days.[83]
Metformin has acid dissociation constant values (pKa) of 2.8 and 11.5, so exists very largely as the hydrophilic cationic species at physiological pH values. The metformin pKa values make metformin a stronger base than most other basic drugs with less than 0.01% nonionized in blood. Furthermore, the lipid solubility of the nonionized species is slight as shown by its low logP value [log(10) of the distribution coefficient of the nonionized form between octanol and water] of -1.43. These chemical parameters indicate low lipophilicity and, consequently, rapid passive diffusion of metformin through cell membranes is unlikely. The logP of metformin is less than that of phenformin (-0.84) because two methyl substituents on metformin impart lesser lipophilicity than the larger phenylethyl side chain in phenformin. More lipophilic derivatives of metformin are presently being investigated with the aim of producing prodrugs with better oral absorption than metformin itself.[104]
Metformin is not metabolized. It is cleared from the body by tubular secretion and excreted unchanged in the urine; metformin is undetectable in blood plasma within 24 hours of a single oral dose.[83][105] The average elimination half-life in plasma is 6.2 hours.[83] Metformin is distributed to (and appears to accumulate in) red blood cells, with a much longer elimination half-life: 17.6 hours[83] (reported as ranging from 18.5 to 31.5 hours in a single-dose study of nondiabetic people).[105]
History
The biguanide class of antidiabetic drugs, which also includes the withdrawn agents phenformin and buformin, originates from the French lilac or goat's rue (Galega officinalis), a plant used in folk medicine for several centuries.[106]

Metformin was first described in the scientific literature in 1922, by Emil Werner and James Bell, as a product in the synthesis of N,N-dimethylguanidine.[99] In 1929, Slotta and Tschesche discovered its sugar-lowering action in rabbits, noting it was the most potent of the biguanide analogs they studied.[107] This result was completely forgotten, as other guanidine analogs, such as the synthalins, took over and were themselves soon overshadowed by insulin.[108]
Interest in metformin, however, picked up at the end of the 1940s. In 1950, metformin, unlike some other similar compounds, was found not to decrease blood pressure and heart rate in animals.[109] That same year, a prominent Philippine physician, Eusebio Y. Garcia,[110] used metformin (he named it Fluamine) to treat influenza; he noted the drug "lowered the blood sugar to minimum physiological limit" and was not toxic. Garcia also believed metformin to have bacteriostatic, antiviral, antimalarial, antipyretic, and analgesic actions.[111] In a series of articles in 1954, Polish pharmacologist Janusz Supniewski[112] was unable to confirm most of these effects, including lowered blood sugar; he did, however, observe some antiviral effects in humans.[113][114]
While training at the Hôpital de la Pitié, French diabetologist Jean Sterne studied the antihyperglycemic properties of galegine, an alkaloid isolated from Galega officinalis, which is related in structure to metformin and had seen brief use as an antidiabetic before the synthalins were developed.[115] Later, working at Laboratoires Aron in Paris, he was prompted by Garcia's report to reinvestigate the blood sugar-lowering activity of metformin and several biguanide analogs. Sterne was the first to try metformin on humans for the treatment of diabetes; he coined the name "Glucophage" (glucose eater) for the drug and published his results in 1957.[108][115]
Metformin became available in the British National Formulary in 1958. It was sold in the UK by a small Aron subsidiary called Rona. [116]
Broad interest in metformin was not rekindled until the withdrawal of the other biguanides in the 1970s. Metformin was approved in Canada in 1972,[117] but did not receive approval by the U.S. Food and Drug Administration (FDA) for type 2 diabetes until 1994.[118] Produced under license by Bristol-Myers Squibb, Glucophage was the first branded formulation of metformin to be marketed in the United States, beginning on March 3, 1995.[119] Generic formulations are now available in several countries, and metformin is believed to have become the most widely prescribed antidiabetic drug in the world.[115]
Formulations

The name "Metformin" is the BAN, USAN and INN for the drug. It is sold under several trade names, including Glucophage XR, Carbophage SR, Riomet, Fortamet, Glumetza, Obimet, Gluformin, Dianben, Diabex, Diaformin, Siofor, Metfogamma and Glifor.
Liquid metformin is sold under the name Riomet in India. Each 5 ml of Riomet is equivalent to the 500-mg tablet form of metformin.[120]
Metformin IR (immediate release) is available in 500, 850, and 1000-mg tablets. All of these are now available as generic drugs in the U.S.
Metformin SR (slow release) or XR (extended release) was introduced in 2004. It is available in 500, 750, and 1000-mg strengths, mainly to counteract the most common gastrointestinal side effects, as well as to increase compliance by reducing pill burden. No difference in effectiveness exists between the two preparations.
Combination with other drugs
When used for type 2 diabetes, metformin is often prescribed in combination with other drugs. Several are available as fixed-dose combinations, also with the purpose of reducing pill burden and making administration simpler and more convenient.[121]
Rosiglitazone
A combination of metformin and rosiglitazone was released in 2002 and sold as Avandamet by GlaxoSmithKline.[122] By 2009 it had become the most popular metformin combination.[123] In 2005, all current stock of Avandamet was seized by the FDA and removed from the market, after inspections showed the factory where it was produced was violating good manufacturing practices.[124] The drug pair continued to be prescribed separately, and Avandamet was available again by the end of that year. A generic formulation of metformin/rosiglitazone from Teva received tentative approval from the FDA, and was expected to reach the market in early 2012.[125] However, following a meta-analysis in 2007 that linked the drug's use to an increased risk of heart attack,[126] concerns were raised over the safety of medicines containing rosiglitazone. In September 2010 the European Medicines Agency (EMA) recommended that the drug be suspended from the European market because the benefits of rosiglitazone no longer outweighed the risks.[127][128] It was withdrawn from the market in the UK and India in 2010,[129] and in New Zealand and South Africa in 2011.[130] From November 2011 until November 2013 the FDA in the U.S.[131] did not allow rosiglitazone or metformin/rosiglitazone to be sold without a prescription; moreover, people were required to be informed of the risks associated with its use, and the drug had to be purchased by mail order through specified pharmacies.[132] In November 2013, the FDA lifted its earlier restrictions on rosiglitazone after reviewing the results of the 2009 RECORD clinical trial (a six-year, open label randomized control trial), which failed to show elevated risk of heart attack or death associated with the drug.[133][134][135]
The combination of metformin and pioglitazone remains available in U.S. and Europe.[136][137]
DPP-4 inhibitors
Dipeptidyl peptidase-4 inhibitors inhibit dipeptidyl peptidase-4 and thus reduce glucagon and blood glucose levels.
DPP-4 inhibitors combined with metformin include a sitagliptin/metformin combination (Janumet) and a saxagliptin combination (Komboglyze/Kombiglyze), and with alogliptin as Kazano.
In Europe, Canada, and elsewhere metformin combined with linagliptin is now sold under the trade name Jentadueto.[138]
Sulfonylureas
Sulfonylureas act by increasing insulin release from the beta cells in the pancreas. Metformin is available combined with the sulfonylureas glipizide (Metaglip) and glibenclamide (US:glyburide) (Glucovance). Generic formulations of metformin/glipizide and metformin/glibenclamide are available (the latter being more popular).[139]
Meglitinide
Meglitinides are similar to sulfonylureas. A repaglinide/metformin combination is sold as Prandimet.
Thiazolidinedione
The thiazolidinedione pioglitazone may be used in combination with metformin (Actoplus Met, Piomet, Politor).
Research
Metformin has been studied in non-alcoholic fatty liver disease (NAFLD)[140] and premature puberty;[141] however these uses are still experimental.[142][143]
Tentative evidence supports an anti-cancer effect for metformin.[144][145]
As of 2015 metformin was under study for its potential effect on slowing aging in the worm C.elegans and the cricket.[146] Its effect on otherwise healthy humans is unknown.[146]
References
- 1 2 3 4 5 Dunn CJ, Peters DH (May 1995). "Metformin. A review of its pharmacological properties and therapeutic use in non-insulin-dependent diabetes mellitus". Drugs. 49 (5): 721–49. doi:10.2165/00003495-199549050-00007. PMID 7601013.
- ↑ Hundal RS, Inzucchi SE (2003). "Metformin: new understandings, new uses". Drugs. 63 (18): 1879–94. doi:10.2165/00003495-200363180-00001. PMID 12930161.
- 1 2 3 4 5 6 7 8 9 10 11 12 13 "Metformin Hydrochloride". The American Society of Health-System Pharmacists. Retrieved Jan 2016. Check date values in:
|access-date=(help) - ↑ Maruthur, NM; Tseng, E; Hutfless, S; Wilson, LM; Suarez-Cuervo, C; Berger, Z; Chu, Y; Iyoha, E; Segal, JB; Bolen, S (19 April 2016). "Diabetes Medications as Monotherapy or Metformin-Based Combination Therapy for Type 2 Diabetes: A Systematic Review and Meta-analysis.". Annals of Internal Medicine. doi:10.7326/M15-2650. PMID 27088241.
- ↑ Clinical Obesity. (2nd ed.). Oxford: John Wiley & Sons. 2008. p. 262. ISBN 9781405143660.
- ↑ Malek, M; Aghili, R; Emami, Z; Khamseh, ME (2013). "Risk of Cancer in Diabetes: The Effect of Metformin." (PDF). ISRN Endocrinology. 2013: 636927. doi:10.1155/2013/636927. PMC 3800579
 . PMID 24224094.
. PMID 24224094. - 1 2 "Type 2 diabetes and metformin. First choice for monotherapy: weak evidence of efficacy but well-known and acceptable adverse effects.". Prescrire international. 23 (154): 269–72. November 2014. PMID 25954799.
- ↑ Triggle, CR; Ding, H (17 December 2015). "Metformin is not just an antihyperglycaemic drug but also has protective effects on the vascular endothelium.". Acta physiologica (Oxford, England). doi:10.1111/apha.12644. PMID 26680745.
- ↑ Lipska KJ, Bailey CJ, Inzucchi SE (June 2011). "Use of metformin in the setting of mild-to-moderate renal insufficiency". Diabetes Care. 34 (6): 1431–7. doi:10.2337/dc10-2361. PMC 3114336. PMID 21617112.
- ↑ Lautatzis, ME; Goulis, DG; Vrontakis, M (November 2013). "Efficacy and safety of metformin during pregnancy in women with gestational diabetes mellitus or polycystic ovary syndrome: a systematic review.". Metabolism: clinical and experimental. 62 (11): 1522–34. doi:10.1016/j.metabol.2013.06.006. PMID 23886298.
- 1 2 3 Fischer, Janos (2010). Analogue-based Drug Discovery II. John Wiley & Sons. pp. 47–49. ISBN 9783527632121.
- ↑ McKee, Mitchell Bebel Stargrove, Jonathan Treasure, Dwight L. (2008). Herb, nutrient, and drug interactions : clinical implications and therapeutic strategies. St. Louis, Mo.: Mosby/Elsevier. p. 217. ISBN 9780323029643.
- ↑ "WHO Model List of EssentialMedicines" (PDF). World Health Organization. October 2013. Retrieved 22 April 2014.
- ↑ "Metformin". Retrieved 11 January 2016.
- ↑ Lord JM, Flight IHK, Norman RJ. Metformin in polycystic ovary syndrome: systematic review and meta-analysis. BMJ. 2003;327(7421):951–3. doi:10.1136/bmj.327.7421.951. PMID 14576245. PMC 259161.
- ↑ Bennett WL, Maruthur NM, Singh S, Segal JB, Wilson LM, Chatterjee R, Marinopoulos SS, Puhan MA, Ranasinghe P, Block L, Nicholson WK, Hutfless S, Bass EB, Bolen S (3 May 2011). "Comparative Effectiveness and Safety of Medications for Type 2 Diabetes: An Update Including New Drugs and 2-Drug Combinations". Annals of Internal Medicine. 154 (9): 602–13. doi:10.7326/0003-4819-154-9-201105030-00336. PMC 3733115. PMID 21403054.
- 1 2 Inzucchi SE, Bergenstal RM, Buse JB, et al. (June 2012). "Management of hyperglycemia in type 2 diabetes: a patient-centered approach: position statement of the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD)". Diabetes Care. 35 (6): 1364–79. doi:10.2337/dc12-0413. PMC 3357214. PMID 22517736.
- ↑ Effect of intensive blood-glucose control with metformin on complications in overweight patients with type 2 diabetes (UKPDS 34). UK Prospective Diabetes Study (UKPDS) Group. Lancet. 1998;352(9131):854–65. doi:10.1016/S0140-6736(98)07037-8. PMID 9742977.
- ↑ Selvin E, Bolen S, Yeh HC, et al. Cardiovascular outcomes in trials of oral diabetes medications: a systematic review. Arch Intern Med. October 2008;168(19):2070–80. doi:10.1001/archinte.168.19.2070. PMID 18955635. PMC 2765722.
- ↑ Groop, Leif; Boussageon, Rémy; Supper, Irène; Bejan-Angoulvant, Theodora; Kellou, Nadir; Cucherat, Michel; Boissel, Jean-Pierre; Kassai, Behrouz; Moreau, Alain; Gueyffier, François; Cornu, Catherine (2012). "Reappraisal of Metformin Efficacy in the Treatment of Type 2 Diabetes: A Meta-Analysis of Randomised Controlled Trials". PLoS Medicine. 9 (4): e1001204. doi:10.1371/journal.pmed.1001204. ISSN 1549-1676. PMC 3323508. PMID 22509138.
- ↑ "ESC Guidelines on diabetes, pre-diabetes, and cardiovascular diseases developed in collaboration with the EASD - Summary". Diab Vasc Dis Res. 11 (3): 133–73. May 2014. doi:10.1177/1479164114525548. PMID 24800783.
- ↑ Qaseem A, Humphrey LL, Sweet DE, Starkey M, Shekelle P (February 2012). "Oral pharmacologic treatment of type 2 diabetes mellitus: a clinical practice guideline from the American College of Physicians". Ann. Intern. Med. 156 (3): 218–31. doi:10.7326/0003-4819-156-3-201202070-00011. PMID 22312141.
- ↑ Hemmingsen B, Schroll JB, Wetterslev J, et al. (July 2014). "Sulfonylurea versus metformin monotherapy in patients with type 2 diabetes: a Cochrane systematic review and meta-analysis of randomized clinical trials and trial sequential analysis". CMAJ Open. 2 (3): E162–75. doi:10.9778/cmajo.20130073. PMC 4185978. PMID 25295236.
- 1 2 Johansen, K. (1999). "Efficacy of metformin in the treatment of NIDDM. Meta-analysis". Diabetes Care. 22 (1): 33–37. doi:10.2337/diacare.22.1.33. ISSN 0149-5992.
- ↑ Golay, A (2007). "Metformin and body weight". International Journal of Obesity. 32 (1): 61–72. doi:10.1038/sj.ijo.0803695. ISSN 0307-0565.
- ↑ Mead, E; Atkinson, G; Richter, B; Metzendorf, MI; Baur, L; Finer, N; Corpeleijn, E; O'Malley, C; Ells, LJ (29 November 2016). "Drug interventions for the treatment of obesity in children and adolescents.". The Cochrane database of systematic reviews. 11: CD012436. PMID 27899001.
- 1 2 3 4 Maharani U. Chapter 27: Diabetes Mellitus & Hypoglycemia. In: Papadakis MA, McPhee SJ. CURRENT Medical Diagnosis and Treatment 2010. 49th ed. McGraw-Hill Medical; 2009. ISBN 0-07-162444-9. p. 1092–93.
- 1 2 3 Bolen S, Feldman L, Vassy J, et al. Systematic review: comparative effectiveness and safety of oral medications for type 2 diabetes mellitus. Ann Intern Med. 2007;147(6):386–99. doi:10.7326/0003-4819-147-6-200709180-00178. PMID 17638715.
- ↑ DiPiro, Joseph T.; Talbert, Robert L.; Yee, Gary C.; Matzke, Gary R.; Wells, Barbara G.; Posey, L. Michael. Pharmacotherapy: a pathophysiologic approach. New York: McGraw-Hill; 2005. ISBN 0-07-141613-7.
- ↑ "Glucophage package insert". Princeton, NJ: Bristol-Myers Squibb Company; 2009.
- ↑ Knowler WC, Barrett-Connor E, Fowler SE, et al. Reduction in the incidence of type 2 diabetes with lifestyle intervention or metformin. N Engl J Med. February 2002;346(6):393–403. doi:10.1056/NEJMoa012512. PMID 11832527.
- ↑ Knowler WC, Fowler SE, Hamman RF, et al. 10-year follow-up of diabetes incidence and weight loss in the Diabetes Prevention Program Outcomes Study. Lancet. November 2009;374(9702):1677–86. doi:10.1016/S0140-6736(09)61457-4. PMID 19878986.
- ↑ Lilly M, Godwin M. Treating prediabetes with metformin: systematic review and meta-analysis. Can Fam Physician. April 2009;55(4):363–9. PMID 19366942.
- ↑ Kidson W. Polycystic ovary syndrome: a new direction in treatment. Med J Aust. November 1998;169(10):537–40. PMID 9861912.
- ↑ Velazquez EM, Mendoza S, Hamer T, Sosa F, Glueck CJ. Metformin therapy in polycystic ovary syndrome reduces hyperinsulinemia, insulin resistance, hyperandrogenemia, and systolic blood pressure, while facilitating normal menses and pregnancy. Metab Clin Exp. May 1994;43(5):647–54. doi:10.1016/0026-0495(94)90209-7. PMID 8177055.
- ↑ Teede H. Insulin sensitizers in polycystic ovary syndrome. In: Kovács GT, Norman RW. Polycystic ovary syndrome. Cambridge, UK: Cambridge University Press; 2007. ISBN 0-521-84849-0. p. 65–81.
- ↑ National Collaborating Centre for Women's and Children's Health. Fertility: assessment and treatment for people with fertility problems [pdf]. London: Royal College of Obstetricians and Gynaecologists; 2004. ISBN 1-900364-97-2. p. 58–9.
- ↑ Legro RS, Barnhart HX, Schlaff WD, et al. Clomiphene, metformin, or both for infertility in the polycystic ovary syndrome. N Engl J Med. February 2007;356(6):551–66. doi:10.1056/NEJMoa063971. PMID 17287476.
- ↑ Moll E, Bossuyt PM, Korevaar JC, Lambalk CB, van der Veen F. Effect of clomifene citrate plus metformin and clomifene citrate plus placebo on induction of ovulation in women with newly diagnosed polycystic ovary syndrome: randomised double blind clinical trial. BMJ. June 2006;332(7556):1485. doi:10.1136/bmj.38867.631551.55. PMID 16769748.
- ↑ Balen A. Royal College of Obstetricians and Gynaecologists. Metformin therapy for the management of infertility in women with polycystic ovary syndrome [PDF]; December 2008 [Retrieved 2009-12-13].
- ↑ The Thessaloniki ESHRE/ASRM-Sponsored PCOS Consensus Workshop Group. Consensus on infertility treatment related to polycystic ovary syndrome. Hum Reprod. March 2008;23(3):462–77. doi:10.1093/humrep/dem426. PMID 18308833.
- ↑ Palomba S, Pasquali R, Orio F, Nestler JE. Clomiphene citrate, metformin or both as first-step approach in treating anovulatory infertility in patients with polycystic ovary syndrome (PCOS): a systematic review of head-to-head randomized controlled studies and meta-analysis. Clin. Endocrinol. (Oxf). February 2009;70(2):311–21. doi:10.1111/j.1365-2265.2008.03369.x. PMID 18691273.
- ↑ Al-Inany H, Johnson N. Drugs for anovulatory infertility in polycystic ovary syndrome. BMJ. June 2006;332(7556):1461–2. doi:10.1136/bmj.332.7556.1461. PMID 16793784.
- ↑ Radosh L. Drug treatments for polycystic ovary syndrome. Am Fam Physician. April 2009;79(8):671–6. PMID 19405411.
- ↑ Tang T, Lord JM, Norman RJ, Yasmin E, Balen AH. Insulin-sensitising drugs (metformin, rosiglitazone, pioglitazone, D-chiro-inositol) for women with polycystic ovary syndrome, oligo amenorrhoea and subfertility. Cochrane Database Syst Rev. 2009;(4):CD003053. doi:10.1002/14651858.CD003053.pub3. PMID 19821299.
- ↑ Ghazeeri, GS; Nassar, AH; Younes, Z; Awwad, JT (June 2012). "Pregnancy outcomes and the effect of metformin treatment in women with polycystic ovary syndrome: an overview.". Acta Obstetricia et Gynecologica Scandinavica. 91 (6): 658–78. PMID 22375613.
- ↑ Kumar, Pratap; Khan, Kashif (2012-01-01). "Effects of metformin use in pregnant patients with polycystic ovary syndrome". Journal of Human Reproductive Sciences. 5 (2): 166–169. doi:10.4103/0974-1208.101012. ISSN 0974-1208. PMC 3493830. PMID 23162354.
- ↑ Nicholson W, Bolen S, Witkop CT, Neale D, Wilson L, Bass E. Benefits and risks of oral diabetes agents compared with insulin in women with gestational diabetes: a systematic review. Obstet Gynecol. January 2009;113(1):193–205. doi:10.1097/AOG.0b013e318190a459. PMID 19104375.
- ↑ Kitwitee, P; Limwattananon, S; Limwattananon, C; Waleekachonlert, O; Ratanachotpanich, T; Phimphilai, M; Nguyen, TV; Pongchaiyakul, C (14 May 2015). "Metformin for the treatment of gestational diabetes: An updated meta-analysis.". Diabetes research and clinical practice. doi:10.1016/j.diabres.2015.05.017. PMID 26117686.
- ↑ Cheung NW. The management of gestational diabetes [pdf]. Vasc Health Risk Manag. 2009;5(1):153–64. doi:10.2147/vhrm.s3405. PMID 19436673. PMC 2672462.
- ↑ Sivalingam, V. N.; Myers, J.; Nicholas, S.; Balen, A. H.; Crosbie, E. J. (2014). "Metformin in reproductive health, pregnancy and gynaecological cancer: established and emerging indications". Human Reproduction Update. 20 (6): 853–868. doi:10.1093/humupd/dmu037. ISSN 1355-4786. PMID 25013215.
- ↑ Jones G, Macklin J, Alexander W. Contraindications to the use of metformin. BMJ. 2003;326(7379):4–5. doi:10.1136/bmj.326.7379.4. PMID 12511434. PMC 1124930.
- ↑ U.S. FDA. Glucophage Prescribing Information for the U.S. [PDF] [Retrieved 2009-12-24].
- ↑ Eurich DT, McAlister FA, Blackburn DF, et al. Benefits and harms of antidiabetic agents in patients with diabetes and heart failure: systematic review. BMJ. 2007;335(7618):497. doi:10.1136/bmj.39314.620174.80. PMID 17761999. PMC 1971204.
- 1 2 Weir J (March 19, 1999). Guidelines with Regard to Metformin-Induced Lactic Acidosis and X-ray Contrast Medium Agents. Royal College of Radiologists. Retrieved October 26, 2007 through the Internet Archive.
- 1 2 Thomsen HS, Morcos SK. Contrast media and the kidney: European Society of Urogenital Radiology (ESUR) guidelines. Br J Radiol. 2003;76(908):513–8. doi:10.1259/bjr/26964464. PMID 12893691.
- ↑ Khurana R, Malik IS. Metformin: safety in cardiac patients. Heart. 2010;96(2):99–102. doi:10.1136/hrt.2009.173773. PMID 19564648.
- ↑ Vigersky RA, Filmore-Nassar A, Glass AR. Thyrotropin suppression by metformin. J Clin Endocrinol Metab. January 2006;91(1):225–7. doi:10.1210/jc.2005-1210. PMID 16219720.
- ↑ Drug Facts and Comparisons 2005. St. Louis, Mo: Facts and Comparisons; October 2004. ISBN 1-57439-193-3.
- ↑ Wulffele MG, Kooy A, Lehert P, Bets D, Ogterop JC, Borger van der Burg B, Donker AJ, Stehouwer CD. Effects of short-term treatment with metformin on serum concentrations of homocysteine, folate and vitamin B12 in type 2 diabetes mellitus: a randomized, placebo-controlled trial. J Intern Med. November 2003;254(5):455–63. doi:10.1046/j.1365-2796.2003.01213.x. PMID 14535967.
- ↑ Andrès E, Noel E, Goichot B. Metformin-associated vitamin B12 deficiency. Arch Intern Med. 2002;162(19):2251–2. doi:10.1001/archinte.162.19.2251-a. PMID 12390080.
- ↑ Gilligan M. Metformin and vitamin B12 deficiency. Arch Intern Med. 2002;162(4):484–5. doi:10.1001/archinte.162.4.484. PMID 11863489.
- ↑ de Jager J, Kooy A, Lehert P, et al. (2010). "Long term treatment with metformin in patients with type 2 diabetes and risk of vitamin B-12 deficiency: randomised placebo controlled trial". BMJ. 340: c2181. doi:10.1136/bmj.c2181. PMC 2874129. PMID 20488910.
- ↑ Ting R, Szeto C, Chan M, Ma K, Chow K. Risk factors of vitamin B(12) deficiency in patients receiving metformin. Arch Intern Med. 2006;166(18):1975–9. doi:10.1001/archinte.166.18.1975. PMID 17030830.
- 1 2 Stang M, Wysowski DK, Butler-Jones D (1999). "Incidence of lactic acidosis in metformin users". Diabetes Care. 22 (6): 925–927. doi:10.2337/diacare.22.6.925. PMID 10372243.
- 1 2 Salpeter S, Greyber E, Pasternak G, Salpeter E. Risk of fatal and nonfatal lactic acidosis with metformin use in type 2 diabetes mellitus: systematic review and meta-analysis. Arch Intern Med. 2003;163(21):2594–602. doi:10.1001/archinte.163.21.2594. PMID 14638559.
- 1 2 Shu AD, Myers Jr MG, Shoelson SE. Chapter 29: Pharmacology of the Endocrine Pancreas. In: Golan ED et al. (eds.). Principles of pharmacology: the pathophysiologic basis of drug therapy. Philadelphia: Lippincott, Williams & Wilkins; 2005. ISBN 0-7817-4678-7. p. 540–41.
- 1 2 3 Kirpichnikov D, McFarlane SI, Sowers JR. Metformin: an update [PDF]. Ann Intern Med. 2002;137(1):25–33. doi:10.7326/0003-4819-137-1-200207020-00009. PMID 12093242.
- ↑ Davis SN. Chapter 60: Insulin, Oral Hypoglycemic Agents, and the Pharmacology of the Endocrine Pancreas. In: Brunton L, Lazo J, Parker K. Goodman & Gilman's The Pharmacological Basis of Therapeutics. 11th ed. New York: McGraw-Hill; 2006. ISBN 978-0-07-142280-2.
- ↑ Spiller HA, Quadrani DA. Toxic effects from metformin exposure. Ann Pharmacother. 2004;38(5):776–80. doi:10.1345/aph.1D468. PMID 15031415.
- 1 2 Forrester MB. Adult metformin ingestions reported to Texas poison control centers, 2000–2006. Hum Exp Toxicol. July 2008;27(7):575–83. doi:10.1177/0960327108090589. PMID 18829734.
- ↑ Gjedde S, Christiansen A, Pedersen SB, Rungby J. Survival following a metformin overdose of 63 g: a case report. Pharmacol Toxicol. 2003;93(2):98–9. doi:10.1034/j.1600-0773.2003.930207.x. PMID 12899672.
- ↑ Nisse P, Mathieu-Nolf M, Deveaux M, Forceville X, Combes A. A fatal case of metformin poisoning. J Toxicol Clin Toxicol. 2003;41(7):1035–6. doi:10.1081/CLT-120026533. PMID 14705855.
- 1 2 Suchard JR, Grotsky TA. Fatal metformin overdose presenting with progressive hyperglycemia. West J Emerg Med. August 2008;9(3):160–4. PMID 19561734.
- 1 2 Teale KF, Devine A, Stewart H, Harper NJ. The management of metformin overdose. Anaesthesia. July 1998;53(7):698–701. doi:10.1046/j.1365-2044.1998.436-az0549.x. PMID 9771180.
- ↑ Spiller HA, Weber JA, Winter ML, Klein-Schwartz W, Hofman M, Gorman SE, Stork CM, Krenzelok EP. Multicenter case series of pediatric metformin ingestion. Ann Pharmacother. December 2000;34(12):1385–8. doi:10.1345/aph.10116. PMID 11144693.
- ↑ Dell'Aglio DM, Perino LJ, Kazzi Z, Abramson J, Schwartz MD, Morgan BW. Acute metformin overdose: examining serum pH, lactate level, and metformin concentrations in survivors versus nonsurvivors: a systematic review of the literature. Ann Emerg Med. December 2009;54(6):818–23. doi:10.1016/j.annemergmed.2009.04.023. PMID 19556031.
- ↑ Lacher M, Hermanns-Clausen M, Haeffner K, Brandis M, Pohl M. Severe metformin intoxication with lactic acidosis in an adolescent. Eur J Pediatr. June 2005;164(6):362–5. doi:10.1007/s00431-005-1634-y. PMID 15729560.
- 1 2 Calello, DP; Liu, KD; Wiegand, TJ; Roberts, DM; Lavergne, V; Gosselin, S; Hoffman, RS; Nolin, TD; Ghannoum, M; Extracorporeal Treatments in Poisoning, Workgroup (9 April 2015). "Extracorporeal Treatment for Metformin Poisoning: Systematic Review and Recommendations From the Extracorporeal Treatments in Poisoning Workgroup.". Critical Care Medicine. 43: 1716–30. doi:10.1097/CCM.0000000000001002. PMID 25860205.
- ↑ Liu A, Coleman SP (2009). "Determination of metformin in human plasma using hydrophilic interaction liquid chromatography-tandem mass spectrometry". J. Chrom. B. 877 (29): 3695–3700. doi:10.1016/j.jchromb.2009.09.020.
- ↑ R. Baselt, Disposition of Toxic Drugs and Chemicals in Man, 8th edition, Biomedical Publications, Foster City, CA, 2008, pp. 939–940.
- ↑ Somogyi A, Stockley C, Keal J, Rolan P, Bochner F. Reduction of metformin renal tubular secretion by cimetidine in man. Br J Clin Pharmacol. May 1987;23(5):545–51. doi:10.1111/j.1365-2125.1987.tb03090.x. PMID 3593625.
- 1 2 3 4 5 6 7 8 Bristol-Myers Squibb. U.S. Food and Drug Administration. Glucophage (metformin hydrochloride tablets) Label Information; August 27, 2008 [Retrieved 2009-12-08].
- ↑ Jayasagar G, Krishna Kumar M, Chandrasekhar K, Madhusudan Rao C, Madhusudan Rao Y. Effect of cephalexin on the pharmacokinetics of metformin in healthy human volunteers. Drug Metabol Drug Interact. 2002;19(1):41–8. doi:10.1515/dmdi.2002.19.1.41. PMID 12222753.
- 1 2 Collier CA, Bruce CR, Smith AC, Lopaschuk G, Dyck DJ. Metformin counters the insulin-induced suppression of fatty acid oxidation and stimulation of triacylglycerol storage in rodent skeletal muscle. Am J Physiol Endocrinol Metab. 2006;291(1):E182–E189. doi:10.1152/ajpendo.00272.2005. PMID 16478780.
- ↑ Hundal R, Krssak M, Dufour S, Laurent D, Lebon V, Chandramouli V, Inzucchi S, Schumann W, Petersen K, Landau B, Shulman G. Mechanism by which metformin reduces glucose production in type 2 diabetes [PDF]. Diabetes. 2000;49(12):2063–9. doi:10.2337/diabetes.49.12.2063. PMID 11118008. PMC 2995498.
- 1 2 3 Rena G, Pearson ER, Sakamoto K (September 2013). "Molecular mechanism of action of metformin: old or new insights?". Diabetologia. 56 (9): 1898–906. doi:10.1007/s00125-013-2991-0. PMC 3737434. PMID 23835523.
- 1 2 Burcelin R (July 2013). "The antidiabetic gutsy role of metformin uncovered?". Gut. 63 (5): 706–707. doi:10.1136/gutjnl-2013-305370. PMID 23840042.
- ↑ Madiraju, Anila K.; Erion, Derek M.; Rahimi, Yasmeen; Zhang, Xian-Man; Braddock, Demetrios T.; Albright, Ronald A.; Prigaro, Brett J.; Wood, John L.; Bhanot, Sanjay; MacDonald, Michael J.; Jurczak, Michael J.; Camporez, Joao-Paulo; Lee, Hui-Young; Cline, Gary W.; Samuel, Varman T.; Kibbey, Richard G.; Shulman, Gerald I. (21 May 2014). "Metformin suppresses gluconeogenesis by inhibiting mitochondrial glycerophosphate dehydrogenase". Nature. 510 (7506): 542–546. doi:10.1038/nature13270.
- ↑ Towler MC, Hardie DG. AMP-activated protein kinase in metabolic control and insulin signaling. Circ Res. 2007;100(3):328–41. doi:10.1161/01.RES.0000256090.42690.05. PMID 17307971.
- ↑ Zhou G, Myers R, Li Y, Chen Y, Shen X, Fenyk-Melody J, Wu M, Ventre J, Doebber T, Fujii N, Musi N, Hirshman M, Goodyear L, Moller D. Role of AMP-activated protein kinase in mechanism of metformin action. J Clin Invest. 2001;108(8):1167–74. doi:10.1172/JCI13505. PMID 11602624. PMC 209533.
- ↑ Kim YD, Park KG, Lee YS, et al. Metformin inhibits hepatic gluconeogenesis through AMP-activated protein kinase-dependent regulation of the orphan nuclear receptor SHP. Diabetes. 2008;57(2):306–14. doi:10.2337/db07-0381. PMID 17909097.
- ↑ Zhang L, He H, Balschi JA. Metformin and phenformin activate AMP-activated protein kinase in the heart by increasing cytosolic AMP concentration. Am J Physiol Heart Circ Physiol. 2007;293(1):H457–66. doi:10.1152/ajpheart.00002.2007. PMID 17369473.
- ↑ Miller RA, Chu Q, Xie J, Foretz M, Viollet B, Birnbaum MJ.. Biguanides suppress hepatic glucagon signalling by decreasing production of cyclic AMP. Nature. 2013 Feb 14;494(7436):256–60. doi:10.1038/nature11808. PMID 23292513.
- ↑ Bailey CJ, Turner RC. Metformin. N Engl J Med. 1996;334(9):574–9. doi:10.1056/NEJM199602293340906. PMID 8569826.
- ↑ Fantus IG, Brosseau R. Mechanism of action of metformin: insulin receptor and postreceptor effects in vitro and in vivo. J Clin Endocrinol Metab. 1986;63(4):898-905. doi:10.1210/jcem-63-4-898. PMID 3745404.
- ↑ Musi N, Hirshman MF, Nygren J, et al. sensitivity/cgi/content/full/51/7/2074 Metformin increases AMP-activated protein kinase activity in skeletal muscle of subjects with type 2 diabetes. Diabetes. 2002;51(7):2074–81. doi:10.2337/diabetes.51.7.2074. PMID 12086935.
- ↑ Saeedi R, Parsons HL, Wambolt RB, et al. Metabolic actions of metformin in the heart can occur by AMPK-independent mechanisms. Am J Physiol Heart Circ Physiol. 2008;294(6):H2497–506. doi:10.1152/ajpheart.00873.2007. PMID 18375721.
- 1 2 Werner E, Bell J. The preparation of methylguanidine, and of ββ-dimethylguanidine by the interaction of dicyandiamide, and methylammonium and dimethylammonium chlorides respectively. J Chem Soc, Transactions. 1922;121:1790–5. doi:10.1039/CT9222101790.
- ↑ Shapiro SL, Parrino VA, Freedman L. Hypoglycemic Agents. I Chemical Properties of β-Phenethylbiguanide. A New Hypoglycemic Agent. J Am Chem Soc. 1959;81(9):2220–5. doi:10.1021/ja01518a052.
- ↑ Procédé de préparation de chlorhydrate de diméthylbiguanide. Patent FR 2322860. 1975. French.
- ↑ Pharmaceutical Manufacturing Encyclopedia (Sittig's Pharmaceutical Manufacturing Encyclopedia). 3rd ed. Vol. 3. Norwich, NY: William Andrew; 2007. ISBN 0-8155-1526-X. p. 2208.
- 1 2 Heller JB. Metformin overdose in dogs and cats. Veterinary Medicine. 2007;(April):231–233.
- ↑ Garry G. Graham, Jeroen Punt, Manit Arora, Richard O. Day, Matthew P. Doogue, Janna K. Duong, Timothy J. Furlong, Jerry R. Greenfield, Louise C. Greenup, Carl M. Kirkpatrick, John E. Ray, Peter Timmins and Kenneth M. Williams.. Clinical Pharmacokinetics of Metformin.. Clin Pharmacokinet. 2011;50(2):81-98. doi:10.2165/11534750-000000000-00000.
- 1 2 Robert F, Fendri S, Hary L, Lacroix C, Andréjak M, Lalau JD. Kinetics of plasma and erythrocyte metformin after acute administration in healthy subjects. Diabetes Metab. June 2003;29(3):279–83. doi:10.1016/s1262-3636(07)70037-x. PMID 12909816.
- ↑ Witters L. The blooming of the French lilac. J Clin Invest. 2001;108(8):1105–7. doi:10.1172/JCI14178. PMID 11602616. PMC 209536.
- ↑ See Chemical Abstracts, v.23, 42772 (1929) K. H. Slotta, R. Tschesche. Uber Biguanide. II. Die Blutzuckersenkende Wirkung der Biguanides. Berichte der Deutschen Chemischen Gesellschaft B: Abhandlungen. 1929;62:1398–1405. doi:10.1002/cber.19290620605.
- 1 2 Campbell IW. Metformin—life begins at 50: A symposium held on the occasion of the 43rd Annual Meeting of the European Association for the Study of Diabetes, Amsterdam, The Netherlands, September 2007. The British Journal of Diabetes & Vascular Disease. 2007;7:247–252. doi:10.1177/14746514070070051001.
- ↑ Dawes GS, Mott JC. Circulatory and respiratory reflexes caused by aromatic guanidines. Br J Pharmacol Chemother. March 1950;5(1):65–76. doi:10.1111/j.1476-5381.1950.tb00578.x. PMID 15405470.
- ↑ About Eusebio Y. Garcia, see: Carteciano J. Philippines Department of Science and Technology. Search for DOST-NRCP Dr. Eusebio Y. Garcia Award; 2005 [Retrieved 2009-12-05].
- ↑ Quoted from Chemical Abstracts, v.45, 24828 (1951) Garcia EY. Fluamine, a new synthetic analgesic and antiflu drug. J Philippine Med Assoc. 1950;26:287–93.
- ↑ About Janusz Supniewski, see: Wołkow PP, Korbut R. Pharmacology at the Jagiellonian University in Kracow, short review of contribution to global science and cardiovascular research through 400 years of history [pdf]. J Physiol Pharmacol. April 2006 [Retrieved 2009-12-05];57 Suppl 1:119–36. PMID 16766803.
- ↑ See Chemical Abstracts, v. 52, 22272 (1958) Supniewski J, Chrusciel T. [N-dimethyl-di-guanide and its biological properties.]. Arch Immunol Ther Exp (Warsz). 1954;2:1–15. Polish. PMID 13269290.
- ↑ Quoted from Chemical Abstracts, v.49, 74699 (1955) Supniewski J, Krupinska, J. [Effect of biguanide derivatives on experimental cowpox in rabbits.]. Bulletin de l'Academie Polonaise des Sciences, Classe 3: Mathematique, Astronomie, Physique, Chimie, Geologie et Geographie. 1954;2(Classe II):161–5. French.
- 1 2 3 Bailey CJ, Day C. Metformin: its botanical background. Practical Diabetes International. 2004;21(3):115–7. doi:10.1002/pdi.606.
- ↑ Hadden DR. Goat's rue – French lilac – Italian fitch – Spanish sainfoin: gallega officinalis and metformin: the Edinburgh connection. J R Coll Physicians Edinb. October 2005;35(3):258–60. PMID 16402501.
- ↑ Lucis OJ. The status of metformin in Canada. Can Med Assoc J. January 1983;128(1):24–6. PMID 6847752.
- ↑ Susan M. Cruzan (December 30, 1994). "FDA Approves New Diabetes Drug" (Press release). U.S. Food and Drug Administration. Archived from the original on September 29, 2007. Retrieved 2007-01-06.
- ↑ Glucophage Label and Approval History. U.S. Food and Drug Administration. Retrieved January 8, 2007. Data available for download on FDA website.
- ↑ "Metformin". rxwiki. 9 July 2012.
- ↑ Bailey CJ, Day C. Fixed-dose single tablet antidiabetic combinations. Diabetes Obes Metab. June 2009;11(6):527–33. doi:10.1111/j.1463-1326.2008.00993.x. PMID 19175373.
- ↑ "FDA Approves GlaxoSmithKline's Avandamet (rosiglitazone maleate and metformin HCl), The Latest Advancement in the Treatment of Type 2 Diabetes" (Press release). GlaxoSmithKline. October 12, 2002. Retrieved 2006-12-27.
- ↑ "2009 Top 200 branded drugs by total prescriptions" (PDF). (96.5 KB). Drug Topics (June 17, 2010). Retrieved September 2, 2010.
- ↑ "Questions and Answers about the Seizure of Paxil CR and Avandamet" (Press release). U.S. Food and Drug Administration. March 4, 2005. Archived from the original on October 14, 2007. Retrieved 2006-12-27.
- ↑ "Teva Pharm announces settlement of generic Avandia, Avandamet, and Avandaryl litigation with GlaxoSmithKline" (Press release). Reuters. September 27, 2007. Retrieved 2009-02-17.
- ↑ Nissen SE, Wolski K (2007). "Effect of rosiglitazone on the risk of myocardial infarction and death from cardiovascular causes". N. Engl. J. Med. 356 (24): 2457–71. doi:10.1056/NEJMoa072761. PMID 17517853.
- ↑ "European Medicines Agency recommends suspension of Avandia, Avandamet and Avaglim". News and Events. European Medicines Agency.
- ↑ "Call to 'suspend' diabetes drug". BBC News. 2010-09-23.
- ↑ "Drugs banned in India". Central Drugs Standard Control Organization, Dte.GHS, Ministry of Health and Family Welfare, Government of India. Retrieved 2013-09-17.
- ↑ "Diabetes drug withdrawn". Stuff.co.nz. NZPA. 17 February 2011. Retrieved 5 November 2011.
- ↑ Gardiner Harris (February 19, 2010). "Controversial Diabetes Drug Harms Heart, U.S. Concludes". New York Times.
- ↑ "Most Popular E-mail Newsletter". USA Today. 2011-05-24.
- ↑ "Glaxo's Avandia Cleared From Sales Restrictions by FDA". Bloomberg.
- ↑ U.S. Food and Drug Administration (November 25, 2013). "FDA requires removal of certain restrictions on the diabetes drug Avandia".
- ↑ "US agency reverses stance on controversial diabetes drug".
- ↑ "European Medicines Agency - Human medicines - CHMP summary of positive opinion for Pioglitazone ratiopharm".
- ↑ Actoplus Met (pioglitazone and metformin) fixed-dose combination tablets
- ↑ Jentadueto at the European Medicines Agency. First published 25/05/2012
- ↑ ""The Use of Medicines in the United States: Review of 2010"" (PDF). (1.79 MB). IMS Institute for Healthcare Informatics (April 2011). Retrieved April 28, 2011.
- ↑ Marchesini G, Brizi M, Bianchi G, Tomassetti S, Zoli M, Melchionda N. Metformin in non-alcoholic steatohepatitis. Lancet. 2001;358(9285):893–4. doi:10.1016/S0140-6736(01)06042-1. PMID 11567710.
- ↑ Ibáñez L, Ong K, Valls C, Marcos MV, Dunger DB, de Zegher F. Metformin treatment to prevent early puberty in girls with precocious pubarche. J Clin Endocrinol Metab. 2006;91(8):2888–91. doi:10.1210/jc.2006-0336. PMID 16684823.
- ↑ Angelico F, Burattin M, Alessandri C, Del Ben M, Lirussi F. Drugs improving insulin resistance for non-alcoholic fatty liver disease and/or non-alcoholic steatohepatitis. Cochrane Database Syst Rev. January 2007;24(1):CD005166. doi:10.1002/14651858.CD005166.pub2. PMID 17253544.
- ↑ Socha P, Horvath A, Vajro P, Dziechciarz P, Dhawan A, Szajewska H. Pharmacological interventions for nonalcoholic fatty liver disease in adults and in children: a systematic review. J Pediatr Gastroenterol Nutr. May 2009;48(5):587–96. doi:10.1097/MPG.0b013e31818e04d1. PMID 19412008.
- ↑ Ben Sahra I, Le Marchand Brustel Y, Tanti JF, Bost F. Metformin in cancer therapy: a new perspective for an old antidiabetic drug?. Mol Cancer Therapeutics. May 2010;9(5):1092–99. doi:10.1158/1535-7163.MCT-09-1186. PMID 20442309.
- ↑ Malek, M; Aghili, R; Emami, Z; Khamseh, ME (2013). "Risk of Cancer in Diabetes: The Effect of Metformin.". ISRN endocrinology. 2013: 636927. doi:10.1155/2013/636927. PMC 3800579. PMID 24224094.
- 1 2 Pryor, R; Cabreiro, F (1 November 2015). "Repurposing metformin: an old drug with new tricks in its binding pockets.". The Biochemical Journal. 471 (3): 307–22. doi:10.1042/bj20150497. PMID 26475449.
External links
| Wikimedia Commons has media related to Metformin. |