Klatskin tumor
| Klatskin tumor | |
|---|---|
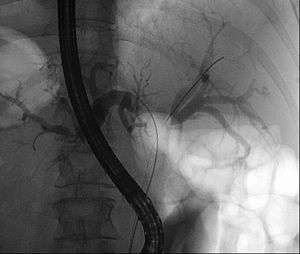 | |
| Klatskin tumor during ERCP. In the left and right biliary system wires were placed. Both parts were injected through a tube with contrast. The lack of contrast in the area of the confluence is clearly visible. | |
| Classification and external resources | |
| Specialty | oncology |
| ICD-10 | C24.0C24.8 |
| ICD-9-CM | 156.1 |
| ICD-O | M8162/3 |
| DiseasesDB | 31517 |
| eMedicine | med/2705 |
| MeSH | D018285 |
A Klatskin tumor (or hilar cholangiocarcinoma) is a cholangiocarcinoma (cancer of the biliary tree) occurring at the confluence of the right and left hepatic bile ducts. It is named after Dr. Gerald Klatskin.[1]
Treatment and prognosis

Because of their location, these tumors tend to become symptomatic late in their development and therefore are not usually resectable at the time of presentation. This is variable as, due to obstruction, jaundice may present early and compel the patient to seek help. Complete resection of the tumor offers hope of long-term survival, and of late there has been renewed interest in liver transplantation from deceased donors along with adjuvant therapy. Prognosis remains poor today.
Cause
The etiology of cholangiocarcinoma has not been clearly defined. A number of pathologic conditions, however, resulting in either acute or chronic biliary tract epithelial injury may predispose to malignant change. Primary sclerosing cholangitis, an idiopathic inflammatory condition of the biliary tree, has been clearly associated with the development of cholangiocarcinoma in up to 40% of patients. Congenital biliary cystic disease, such as choledochal cysts or Caroli's disease, has also been associated with malignant transformation in up to 25% of cases. These conditions appear to be related to an anomalous pancreatico-biliary duct junction and, perhaps, are related to the reflux of pancreatic secretions into the bile duct. Chronic biliary tract parasitic infection, seen commonly in Southeast Asia due to Clonorchis sinensis and Opisthorchis viverrini, has also been identified as a risk factor. Although gallstones and cholecystectomy are not thought to be associated with an increased incidence of cholangiocarcinoma, hepatolithiasis and choledocholithiasis may predispose to malignant change. Further, industrial exposure to asbestos and nitrosamines, and the use of the radiologic contrast agent, Thorotrast (thorium dioxide), are considered to be risk factors for the development of cholangiocarcinoma.
Epidemiology
Approximately 15,000 new cases of liver and biliary tract carcinoma are diagnosed annually in the United States, with roughly 10% of these cases being Klatskin tumors. Cholangiocarcinoma accounts for approximately 2% of all cancer diagnoses, with an overall incidence of 1.2/100,000 individuals. Two-thirds of cases occur in patients over the age of 65, with a near ten-fold increase in patients over 80 years of age. The incidence is similar in both men and women.
References
- ↑ Fenster LF (Jan–Feb 1979). "Gerald Klatskin". Yale J Biol Med. 52 (1): 1–3. PMC 2595709
 .
.
- VIDEO - Hilar Cholangiocarcinoma, Klatskin Tumor presented by Fumito Ito, MD, PhD at the University of Wisconsin School of Medicine and Public Health. (2007)
- KLATSKIN G (1965). "Adenocarcinoma of the hepatic duct at its bifurcation within the porta hepatis. An unusual tumor with distinctive clinical and pathological features". Am. J. Med. 38 (2): 241–56. doi:10.1016/0002-9343(65)90178-6. PMID 14256720.
- PatientPlus Article