Breast hypertrophy
| Breast hypertrophy | |
|---|---|
 | |
| Classification and external resources | |
| Specialty | Gynecology, endocrinology |
| ICD-10 | N62 |
| ICD-9-CM | 611.1 |
| DiseasesDB | 1628 |
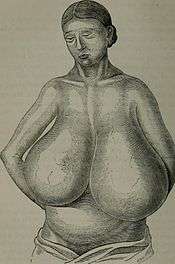
Hypertrophy of the breast (macromastia and gigantomastia) is a rare medical condition of the breast connective tissues. The indication is a breast weight that exceeds approximately 3% of the total body weight.[1] There are varying definitions of what is considered to be excessive breast tissue, that is the expected breast tissue plus extraordinary breast tissue, ranging from as little as 0.6 kilograms (1.3 lb) up to 2.5 kilograms (5.5 lb) with most physicians defining macromastia as excessive tissue of over 1.5 kilograms (3.3 lb). Some resources distinguish between macromastia (Greek, macro: large, mastos: breast), where excessive tissue is less than 2.5 kg, and gigantomastia (Greek, gigantikos: giant), where excessive tissue is more than 2.5 kg.[2][3] The enlargement can cause muscular discomfort and over-stretching of the skin envelope, which can lead in some cases to ulceration.[4] Hypertrophy of the breast tissues might be caused by increased histologic sensitivity to certain hormones such as female sex hormones, prolactin, and growth factors; or an abnormally elevated hormone(s) level in the blood, or both.[5] Breast hypertrophy is a benign progressive enlargement, which can occur in both breasts (bilateral) or only in one breast (unilateral). It was first scientifically described in 1648.[6]
Description and types
Hypertrophy of the breast can affect the breasts equally, but usually affects one breast more than the other, thereby causing asymmetry, when one breast is larger than the other. The condition can also individually affect the nipples and areola instead of or in addition to the entire breast. The effect can produce a minor size variation to an extremely large breast asymmetry. Breast hypertrophy is classified in one of five ways: as either pubertal (virginal hypertrophy), gestational (gravid macromastia), in adult women without any obvious cause, associated with penicillamine therapy, and associated with extreme obesity.[4]
Virginal breast hypertrophy



When gigantomastia occurs in young women during puberty, the medical condition is known as juvenile macromastia or juvenile gigantomastia and sometimes as virginal breast hypertrophy or virginal mammary hypertrophy. Along with the excessive breast size, other symptoms include red, itchy lesions and pain in the breasts. A diagnosis is made when an adolescent's breasts grow rapidly and achieve great weight usually soon after her first menstrual period. Some doctors suggest that the rapid breast development occurs before the onset of menstruation.[10]
Some women with virginal breast hypertrophy experience breast growth at a steady rate for several years, after which the breasts rapidly develop exceeding normal growth. Some adolescent females experience minimal or negligible breast growth until their breasts suddenly grow very rapidly in a short period of time. This may cause considerable physical discomfort. Women suffering VBH often experience an excessive growth of their nipples as well. In severe cases of VBH, hypertrophy of the clitoris occurs.
At the onset of puberty, some females with who have experienced little or no breast development can reportedly reach three or more cup sizes within a few days (see below).[11]
Gestational breast hypertrophy


This same effect can also occur at the onset of pregnancy or between the 16th to 20th week of gestation. When the swelling in the connective tissue occurs after birth, it can negatively impact long term milk supply.[11] The swelling increases with each subsequent pregnancy.
The extremely rapid growth of the breasts can result in intense heat. The woman's breasts can generate extraordinary discomfort, turning feverish, red, itchy, and even causing the skin to peel. The swelling can suppress the milk supply, pinching off the milk ducts, and leading to mastitis.[11]
Gestational gigantomastia is estimated to in 1 out of every 28,000 to 100,000 pregnancies.[14][15] Only 100 cases have been reported in the medical literature.
Breast hypertrophy in infancy

There are case reports of gigantomastia occurring in infants as well.[16][17]
Causes
The underlying cause of the rapidly growing breast connective tissue, resulting in gigantic proportions, has not been well-elucidated. However, proposed factors have included increased levels/expression of or heightened sensitivity to certain hormones (e.g., estrogen, progesterone, and prolactin)[18] and/or growth factors (e.g., hepatic growth factor, insulin-like growth factor 1, and epidermal growth factor) in the breasts.[19][20] Macromastic breasts are reported to be composed mainly of adipose and fibrous tissue, while glandular tissue remains essentially stable.[21]
Macromastia occurs in approximately half of women with aromatase excess syndrome (a condition of hyperestrogenism).[22][23] Hyperprolactinemia has been reported as a cause of some cases of macromastia.[24][25] Macromastia has also been associated with hypercalcemia (which is thought to be due to excessive production of parathyroid hormone-related protein) and, rarely, systemic lupus erythematosus[21] and pseudoangiomatous stromal hyperplasia.[26] It is also notable that approximately two-thirds of women with macromastia are obese.[21] Aside from aromatase (as in aromatase excess syndrome), at least two other genetic mutations (one in PTEN) have been implicated in causing macromastia.[27][28]
A handful of drugs have been associated with gigantomastia, including penicillamine, bucillamine, neothetazone, ciclosporin, and indinavir.[21][29]
Treatment
Medical treatment has not proven consistently effective. Medical regimens have included tamoxifen,[30] progesterone, bromocriptine, the gonadotropin-releasing hormone agonist leuprolide, and testosterone. Gestational macromastia has been treated with breast reduction drugs alone without surgery.[31] Surgical therapy includes reduction mammaplasty and mastectomy.[32] However, breast reduction is not clinically indicated unless at least 1.8 kg (4 lb) of tissue per breast needs to be removed.[33] In the majority of cases of macromastia, surgery is medically unnecessary, depending on body height. Topical treatment includes regimens of ice to cool the breasts.[11]
Treatment of hyperprolactinemia-associated macromastia with D2 receptor agonists such as bromocriptine and cabergoline has been found to be effective in some, but not all cases.[34][35] Danazol, an antiestrogen and weak androgen, has also been found to be effective in the treatment of macromastia.[36]
When hypertrophy occurs in adolescence, noninvasive treatments, including pharmaceutical treatment, hormone therapy, and steroid use are not usually recommended due to known and unknown side effects. Once a girl's breast growth rate has stabilized, breast reduction may be an appropriate choice. In some instances after aggressive or surgical treatment, the breast may continue to grow or re-grow, a complete mastectomy may be recommended as a last resort.
Pregnancy is recognized as the second most common reason for hypertrophy. When secondary to pregnancy, it may resolve itself without treatment after the pregnancy ends.[37]
Reported instances
Gigantomastia


One early and extreme case study of gigantomastia dates to 1670. The patient died four months after the onset of enlargement. One breast removed after the woman's death weighed 29 kg (64 lb).[38]
On April 17, 1848, a 42-year-old woman named Lu-shi was treated for hypertrophy in a Chinese hospital. She was treated by a missionary physician. On December 24, 1849, the left breast, measuring 67 cm (26.5 in) in circumference, and weighing 2.7 kg (6 lb), was removed in a procedure lasting three and a half minutes. The right breast was removed one month later. It measured 61 cm (24 in) in circumference and weighed 2.5 kg (5.5 lb).[39]
In 2005, a woman reported that her breasts grew at puberty from nothing to a C cup in one month. When she became pregnant for the first time, her breasts increased two cup sizes in a few days. Immediately after her first birth, her breasts grew three cup sizes. After her second child was born, her breasts increased six cup sizes. After her third childbirth, they grew 10 cup sizes, and after her fourth child was born, they grew nine cup sizes. In this instance, the swelling abated about 10 days after childbirth, but her bra cup size remained E to a G for the next year. About one year postpartum, her breasts rapidly atrophied to AA cup size.[11]
Another extreme case was observed in 2008 in Maria Vittoria Hospital in Turin, Italy, where the amount removed from both breasts was 17.2 kg (38 lb). The growth occurred during puberty making it a case of juvenile gigantomastia, but the patient did not seek treatment until the age of 29.[40] Another extreme case was observed on August 28, 2003, when a 24-year-old woman was admitted to the Clinical Center Skopje in Macedonia with gigantomastia of pregnancy and the amount later removed from both breasts was 15 kg (33 lb) in total.[41][42] A second case in Macedonia was reported when the breasts of a 30-year-old woman from a remote mountain village in eastern Macedonia suddenly grew to more than 30 kilograms (66 lb) total.[42]
As the disorder becomes more widely known, media reports have increased. French Canadian Isabelle Lanthier appeared on Montel Williams' talk show where she told how her chest grew from 86 cm (34 in) to 133 cm (52.5 in) in five months during her pregnancy. At their largest, one breast weighed 6.8 kg (15 lb) and the other 5.4 kg (12 lb). Her husband custom-made a special bra to support her breasts. In 2007, a Chilean TV station covered the story of 32-year-old Jasna Galleguillos from Antofagasta, who experienced ongoing back pain, making everyday tasks very difficult to perform. She underwent breast reduction surgery to relieve her pain. Surgeons removed 4.25 kilograms (9.4 lb) from one breast and 3.33 kilograms (7.3 lb) from the other breast.[43]
On October 29, 2009, the Philippine television network GMA News and Public Affairs, producers of Wish Ko Lang ("Just My Wish") hosted by Vicky Morales, profiled the story of Pilma Cabrijas, a 30-year-old woman afflicted by gigantomastia. The woman was told by a folk healer that her condition may have been caused by a curse. The measured bust circumference without appropriate bra support was 160 cm (63 in). The weight of her breasts was not reported in detail, but seemed to weigh "as much as two children." She had breast reduction surgery performed, but her breasts regrew. The producers of Wish Ko Lang paid for additional surgery.[44]
Virginal breast hypertrophy
In 1993, the Japanese journal Surgery Today reported on the case of a 12-year-old girl. Only 152 centimetres (60 in) tall and weighing 43 kilograms (95 lb), her breasts began to develop at age 11 before the onset of menstruation. Over the next eight months, both breasts grew abnormally large, and physicians treating her found that her physiological development was normal except for her breasts. The weight produced by their symmetrical and massive enlargement resulted in marked curvature of the spine. Lab tests of her blood for hormones and biochemical substances showed normal values, though tests revealed that it might have been caused by hypersensitivity to estrogen. She underwent a bilateral reduction mammoplasty. Surgeons removed 2 kilograms (4.4 lb) of tissue from her right breast and 1.9 kilograms (4.2 lb) from her left breast. She was administered tamoxifen afterward to suppress breast regrowth.[45]
A more severe case of virginal breast hypertrophy of an 11-year-old girl was reported in 2008. The breasts had begun to grow rapidly at puberty and had reached the point of causing physical impairment and respiratory compromise after one year. The skin was intact without any ulcerations. Blood chemistry and endocrine investigation was normal. A bilateral reduction mammaplasty with free nipple grafts was performed. 6 kg of the right breast and 6.5 kg of the left breast removed, resulting in a removal of 12.5 kg of tissue in all (24% of the total body weight).[46]
Society and culture
Extremely large breasts, also known as macromastia or gigantomastia, are a source of considerable attention. Some women try to hide or mask their breasts with special clothing, including minimizing bras. Women with this condition may be subject to psychological problems due to unwanted attention and/or harassment. Depression is common among sufferers.
In the case of a 12-year-old Japanese girl reported in 1993, her "massively enlarged" breasts caused her "intense psychological problems, incapacitating her in school activities and social relations."[45] Actress Soleil Moon Frye, who starred as a child in the sitcom Punky Brewster, reported in an interview with People magazine that boys taunted her, calling her "Hey, Punky Boobster!" It affected her professional and social life negatively. "People started to think of me as a bimbo," she said in the interview. "I couldn't sit up straight without people looking at me like I was a prostitute," Frye said.[47]
Finding large bra sizes and styles that fit is challenging. Also, larger bras are more costly, challenging to find, and unflattering to the wearer. Ill-fitting bras with narrow straps can cause chronic irritation, redness, and indentations in the shoulders. Skin rashes under the breasts are common, particularly during warm weather. Heavy breasts may cause headaches, neck pain, upper and lower back pain, and numbness or tingling in the fingers.
Many definitions of macromastia and gigantomastia are based on the term of "excessive breast tissue", and are therefore somewhat arbitrary.
Medical insurance coverage
Insurance companies in the United States typically require the physician to provide evidence that a woman's large breasts cause headaches or back and neck pain before they will pay for reduction mammoplasty. Insurance companies also mandate a woman who is overweight, which is often the case with gigantomastia, to first lose a certain amount of weight. They also commonly require the patient to try alternative treatments like physical therapy for a year or more.[48] A plastic surgeon in Seattle, Dr. Phil Haeck, told a reporter that most of his breast reduction patients pay their own way. "I’ve had people finance it; I’ve had people get second mortgages, take out home equity loans."[48]
See also
References
- ↑ Dafydd, H.; Roehl, K.R.; Phillips, L.G.; Dancey, A.; Peart, F.; Shokrollahi, K. (2011). "Redefining gigantomastia". Journal of Plastic, Reconstructive & Aesthetic Surgery. 64 (2): 160–3. doi:10.1016/j.bjps.2010.04.043. PMID 20965141.
- ↑ To Wo Chiu (2011). Stone's Plastic Surgery Facts and Figures (3rd ed.). Cambridge University Press. p. 188.
- ↑ Syed A. Hoda; Edi Brogi; Fred Koerner; Paul Peter Rosen (5 February 2014). Rosen's Breast Pathology. Wolters Kluwer Health. pp. 152–. ISBN 978-1-4698-7070-0.
- 1 2 Note: the criterium of >600g is used with the term "macromastia" in this source: Sharma, K; Nigam, S; Khurana, N; Chaturvedi, KU (2004). "Unilateral gestational macromastia--a rare disorder". The Malaysian journal of pathology. 26 (2): 125–8. PMID 16329566.
- ↑ Ohlsén, L.; Ericsson, O.; Beausang-Linder, M. (1996). "Rapid, massive and unphysiological breast enlargement". European Journal of Plastic Surgery. 19 (6). doi:10.1007/BF00180324.
- ↑ Palmuth, T (1648). "Observations medicuarum centinae tres posthumae". Cent II (Obs 89). Braunschweig.
- ↑ Gentimi, F.; Loupatatzi, A. Ch.; Euthimoglou, K. P.; Michailidou, E. G.; Tzovaras, A. A.; Kaja, A. D.; Poniros, N. S.; Vasiliou, M. V. (2010). "Juvenile Gigantomastia in a 12-Year-Old Girl: A Case Report". Aesthetic Plastic Surgery. 35 (3): 414–417. doi:10.1007/s00266-010-9597-4. ISSN 0364-216X.
- ↑ Menekse, Ebru; Onel, Sefa; Karateke, Faruk; Das, Koray; Bali, İlhan; Bozkurt, Hilmi; Sozen, Selim; Ozdogan, Mehmet (2014). "Virginal Breast Hypertrophy and Symptomatic Treatment: A Case Report". The Journal of Breast Health. 10 (2): 122–124. doi:10.5152/tjbh.2014.1552. ISSN 1306-0945.
- ↑ Dancey, Anne; Khan, M.; Dawson, J.; Peart, F. (2008). "Gigantomastia – a classification and review of the literature". Journal of Plastic, Reconstructive & Aesthetic Surgery. 61 (5): 493–502. doi:10.1016/j.bjps.2007.10.041. ISSN 1748-6815.
- ↑ "Puberty Stages of Development". Ask the Expert FAQs. OBGYN.net. Retrieved 2006-11-21.
- 1 2 3 4 5 Casciola, Cheri (June–July 2005). "Gigantomastia". Leaven. Chandler, Arizona. 41 (3): 62–63. Retrieved October 26, 2009.
- ↑ Wolf, Yoram; Pauzner, David; Groutz, Asnat; Walman, Igal; David, Menachem P. (1995). "Gigantomastia complicating pregnancy: Case report and review of the literature". Acta Obstetricia et Gynecologica Scandinavica. 74 (2): 159–163. doi:10.3109/00016349509008928. ISSN 0001-6349.
- ↑ Eler dos Reis, Pollyana; Blunck Santos, Natalia Quarto; Barbosa Pagio, Fernanda Alves; Chambô, Fabio; Chambô, Danielle; Chambô Filho, Antônio (2014). "Management and Follow-Up of a Case of Gestational Gigantomastia in a Brazilian Hospital". Case Reports in Obstetrics and Gynecology. 2014: 1–4. doi:10.1155/2014/610363. ISSN 2090-6684.
- ↑ Rezai, Shadi; Nakagawa, Jenna T.; Tedesco, John; Chadee, Annika; Gottimukkala, Sri; Mercado, Ray; Henderson, Cassandra E. (2015). "Gestational Gigantomastia Complicating Pregnancy: A Case Report and Review of the Literature". Case Reports in Obstetrics and Gynecology. 2015: 1–10. doi:10.1155/2015/892369. ISSN 2090-6684.
- ↑ Juan, Ph.D., Stephen (January 13, 2007). "Is it true that a woman's breasts can grow enormously overnight?". The Register U.K. Retrieved 2011-08-16.
- 1 2 Mick, G. J.; McCormick, K. L.; Wakimoto, H. (1991). "Massive breast enlargement in an infant girl with central nervous system dysfunction". European Journal of Pediatrics. 150 (3): 154–157. doi:10.1007/BF01963555. ISSN 0340-6199.
- ↑ Zinn, Harry L.; Haller, J. O.; Kedia, Sanjay (1999). "Macromastia in a newborn with Alagille syndrome". Pediatric Radiology. 29 (5): 331–333. doi:10.1007/s002470050601. ISSN 0301-0449.
- ↑ Noczyńska A, Wasikowa R, Myczkowski T (2001). "[Hypersensitivity of estrogen receptors as a cause of gigantomasty in two girls]". Pol. Merkur. Lekarski (in Polish). 11 (66): 507–9. PMID 11899849.
- ↑ Zhong, Aimei; Wang, Guohua; Yang, Jie; Xu, Qijun; Yuan, Quan; Yang, Yanqing; Xia, Yun; Guo, Ke; Horch, Raymund E.; Sun, Jiaming (2014). "Stromal-epithelial cell interactions and alteration of branching morphogenesis in macromastic mammary glands". Journal of Cellular and Molecular Medicine. 18 (7): 1257–1266. doi:10.1111/jcmm.12275. ISSN 1582-1838. PMID 24720804.
- ↑ Kulkarni, Dhananjay; Beechey-Newman, N.; Hamed, H.; Fentiman, I.S. (2006). "Gigantomastia: A problem of local recurrence". The Breast. 15 (1): 100–102. doi:10.1016/j.breast.2005.03.002. ISSN 0960-9776. PMID 16005231.
- 1 2 3 4 Moschella, Francesco; Cordova, Adriana; Toia, Francesca (2016). "Gigantomastia": 239–245. doi:10.1007/978-3-662-46599-8_18.
- ↑ Shozu, Makio; Fukami, Maki; Ogata, Tsutomu (2014). "Understanding the pathological manifestations of aromatase excess syndrome: lessons for clinical diagnosis". Expert Review of Endocrinology & Metabolism. 9 (4): 397–409. doi:10.1586/17446651.2014.926810. ISSN 1744-6651.
- ↑ Martin, Regina M.; Lin, Chin J.; Nishi, Mirian Y.; Billerbeck, Ana Elisa C.; Latronico, Ana Claudia; Russell, David W.; Mendonca, Berenice B. (2003). "Familial Hyperestrogenism in Both Sexes: Clinical, Hormonal, and Molecular Studies of Two Siblings". The Journal of Clinical Endocrinology & Metabolism. 88 (7): 3027–3034. doi:10.1210/jc.2002-021780. ISSN 0021-972X.
- ↑ Rahman GA, Adigun IA, Yusuf IF (2010). "Macromastia: a review of presentation and management". Niger Postgrad Med J. 17 (1): 45–9. PMID 20348982.
- ↑ Dellal, Fatma Dilek; Ozdemir, Didem; Aydin, Cevdet; Kaya, Gulfem; Ersoy, Reyhan; Cakir, Bekir (2016). "Gigantomastia and Macroprolactinemia Responding to Cabergoline Treatment: A Case Report and Minireview of the Literature". Case Reports in Endocrinology. 2016: 1–5. doi:10.1155/2016/3576024. ISSN 2090-6501.
- ↑ Roy, Mélissa; Lee, James; Aldekhayel, Salah; Dionisopoulos, Tassos (2015). "Pseudoangiomatous Stromal Hyperplasia". Plastic and Reconstructive Surgery - Global Open. 3 (9): e501. doi:10.1097/GOX.0000000000000468. ISSN 2169-7574.
- ↑ Li G, Robinson GW, Lesche R, Martinez-Diaz H, Jiang Z, Rozengurt N, Wagner KU, Wu DC, Lane TF, Liu X, Hennighausen L, Wu H (2002). "Conditional loss of PTEN leads to precocious development and neoplasia in the mammary gland". Development. 129 (17): 4159–70. PMID 12163417.
- ↑ Genzer-Nir, Mira; Khayat, Morad; Kogan, Leonid; Cohen, Hector I; Hershkowitz, Miriam; Geiger, Dan; Falik-Zaccai, Tzipora C (2010). "Mammary-digital-nail (MDN) syndrome: a novel phenotype maps to human chromosome 22q12.3–13.1". European Journal of Human Genetics. 18 (6): 662–667. doi:10.1038/ejhg.2009.236. ISSN 1018-4813.
- ↑ David J. Dabbs (2012). Breast Pathology. Elsevier Health Sciences. pp. 19–. ISBN 1-4377-0604-5.
- ↑ Baker, Stephen B.; Burkey, Brooke A.; Thornton, Paul; Larossa, Don (2001). "Juvenile Gigantomastia: Presentation of Four Cases and Review of the Literature". Annals of Plastic Surgery. 46 (5): 517–25; discussion 525–6. doi:10.1097/00000637-200105000-00011. PMID 11352426.
- ↑ Ezem, B. U.; Osuagwu, C. C.; Opara, K. A. (2011). "Gestational gigantomastia with complete resolution in a Nigerian woman". Case Reports. 2011: bcr0120102632. doi:10.1136/bcr.01.2010.2632. PMC 3062818
 . PMID 22707463.
. PMID 22707463. - ↑ Bloom, Sara A.; Nahabedian, Maurice Y. (2008). "Gestational Macromastia: A Medical and Surgical Challenge". The Breast Journal. 14 (5): 492–5. doi:10.1111/j.1524-4741.2008.00628.x. PMID 18657144.
- ↑ Kulkarni, Dhananjay; Beechey-Newman, N.; Hamed, H.; Fentiman, I.S. (2006). "Gigantomastia: A problem of local recurrence". The Breast. 15 (1): 100–2. doi:10.1016/j.breast.2005.03.002. PMID 16005231.
- ↑ Dellal, Fatma Dilek; Aydin, Cevdet; Kaya, Mina Gulfem; Ersoy, Reyhan; Cakir, Bekir (2014). "A case with macroprolactinemia and gigantomastia responding to cabergoline treatment". Endocrine Abstracts. doi:10.1530/endoabs.35.P878. ISSN 1479-6848.
- ↑ Arscott GD, Craig HR, Gabay L (2001). "Failure of bromocriptine therapy to control juvenile mammary hypertrophy". Br J Plast Surg. 54 (8): 720–3. doi:10.1054/bjps.2001.3691. PMID 11728119.
- ↑ Ismail Jatoi; Manfred Kaufmann (11 February 2010). Management of Breast Diseases. Springer Science & Business Media. pp. 47–. ISBN 978-3-540-69743-5.
- ↑ Swelstad, Matthew R.; Swelstad, Brad B.; Rao, Venkat K.; Gutowski, Karol A. (2006). "Management of Gestational Gigantomastia". Plastic and Reconstructive Surgery. 118 (4): 840–8. doi:10.1097/01.prs.0000232364.40958.47. PMID 16980844.
- ↑ Durston, W.; Darston, W. (1669). "An Extract of a Letter Written to the Publisher from Plymouth Novem. 2. 1669. By William Durston Dr. Of Physick; Concerning the Death of the Bigg-Breasted Woman (Discoursed of in Numb. 52.) Together with what Was thereupon Observed in Her Body". Philosophical Transactions of the Royal Society. 4 (45–56): 1068–1069. doi:10.1098/rstl.1669.0048.
- ↑ Qua, Lam (April 17, 1848). "Peter Parker Collection". Medical Historical Library, Cushing/Whitney Medical Library. Retrieved 21 March 2010.
- ↑ Borsetti, G.; Merlino, G.; Bergamin, F.; Cerato, C.; Boltri, M.; Borsetti, M. (2009). "A 38 kg skin-reducing bilateral mastectomy: A unique case". Journal of Plastic, Reconstructive & Aesthetic Surgery. 62: 133–134. doi:10.1016/j.bjps.2008.03.067.
- ↑ Antevski, Borce; Jovkovski, Oliver; Filipovski, Vanja; Banev, Saso (2010). "Extreme gigantomastia in pregnancy: Case report—my experience with two cases in last 5 years". Archives of Gynecology and Obstetrics. 284 (3): 575–8. doi:10.1007/s00404-010-1714-8. PMID 20978777.
- 1 2 "Macedonia faces 'giant' breast problem". Archived from the original on August 3, 2012.
- ↑ "Jasna Galleguillos" (in Spanish). TVN. 2007. Retrieved 22 March 2010.
- ↑ "Pilma's heavy burden". October 29, 2009. Retrieved 22 March 2010.
- 1 2 Morimoto, Tadaoki; Komaki, Kansei; Mori, Toshiaki; Sasa, Mitsunori; Miki, Hitoshi; Inoue, Hiroyuki; Monden, Yasumasa; Nakanishi, Hideki (1993). "Juvenile gigantomastia: Report of a case". Surgery Today. 23 (3): 260–4. doi:10.1007/BF00309238. PMID 8467179.
- ↑ Fiumara, Linda; Gault, David T.; Nel, Mark R.; Lucas, Dominique N.; Courtauld, Elizabeth (2009). "Massive bilateral breast reduction in an 11-year-old girl: 24% ablation of body weight". Journal of Plastic, Reconstructive & Aesthetic Surgery. 62 (8): e263. doi:10.1016/j.bjps.2007.10.053.
- ↑ Rosen, Marjorie (April 26, 1993). "Now I Can Be Free". Vol. 39, No. 16. People Magazine. Retrieved 2009-09-12.
- 1 2 "Too Much of a Good Thing?". Seattle Woman Magazine. Retrieved 2013-03-14.
External links
| Wikimedia Commons has media related to Breast hypertrophy. |
- Touraine, P. (2005). "Breast Inflammatory Gigantomastia in a Context of Immune-Mediated Diseases". Journal of Clinical Endocrinology & Metabolism. 90 (9): 5287–5294. doi:10.1210/jc.2005-0642.
- Oladele, AO; Olabanji, JK; Alabi, GH (2007). "Reduction mammoplasty: The experience in Ile-Ife, Nigeria". Nigerian journal of medicine : journal of the National Association of Resident Doctors of Nigeria. 16 (3): 261–267. PMID 17937167.
- Gigantomasty during pregnancy
- Discovery Health Video - Peggy's Reduction
- Netscher, David T.; Mosharrafa, ALI M.; Laucirica, Rodolfo (1996). "Massive Asymmetric Virginal Breast Hypertrophy". Southern Medical Journal. 89 (4): 434–7. doi:10.1097/00007611-199604000-00019. PMID 8614890.
- U.S.A. Library of Congress - Healthy Breasts: A Primer
- John Blair Deaver (1917). The Breast: Its Anomalies, Its Diseases, and Their Treatment. P. Blakiston's Son & Co.
- Joseph, Jacques (1987). Rhinoplasty and facial plastic surgery with a supplement on mammaplasty and other operations in the field of plastic surgery of the body: an atlas and textbook. Phoenix: Columella Press. p. 755. ISBN 0-9605972-1-2.
- Plummer, Samuel C.; Bump, Warner S. (1927). "Massive Hypertrophy of the Breasts". Annals of Surgery. 85 (1): 61–6. doi:10.1097/00000658-192701000-00008. PMC 1399262. PMID 17865606.
- Warren, John Collins (1900). The International text-book of surgery. Volume II. Saunders. p. 234.
- Erichsen, John Eric (1885). The Science and art of surgery. Vol. II. H. C. Lea's Son & Company. pp. 693–694.
- Ochsner, Albert John (1921). Surgical Diagnosis and Treatment: By American Authors. Lea & Febiger. p. 147.