Drug interaction

A drug interaction is a situation in which a substance (usually another drug) affects the activity of a drug when both are administered together. This action can be synergistic (when the drug's effect is increased) or antagonistic (when the drug's effect is decreased) or a new effect can be produced that neither produces on its own. Typically, interactions between drugs come to mind (drug-drug interaction). However, interactions may also exist between drugs and foods (drug-food interactions), as well as drugs and medicinal plants or herbs (drug-plant interactions). People taking antidepressant drugs such as monoamine oxidase inhibitors should not take food containing tyramine as hypertensive crisis may occur (an example of a drug-food interaction). These interactions may occur out of accidental misuse or due to lack of knowledge about the active ingredients involved in the relevant substances.[1]
 Russ Altman Russ Altman | |
|
|
It is therefore easy to see the importance of these pharmacological interactions in the practice of medicine. If a patient is taking two drugs and one of them increases the effect of the other it is possible that an overdose may occur. The interaction of the two drugs may also increase the risk that side effects will occur. On the other hand, if the action of a drug is reduced it may cease to have any therapeutic use because of under dosage. Notwithstanding the above, on occasion these interactions may be sought in order to obtain an improved therapeutic effect.[3] Examples of this include the use of codeine with paracetamol to increase its analgesic effect. Or the combination of clavulanic acid with amoxicillin in order to overcome bacterial resistance to the antibiotic. It should also be remembered that there are interactions that, from a theoretical standpoint, may occur but in clinical practice have no important repercussions.
The pharmaceutical interactions that are of special interest to the practice of medicine are primarily those that have negative effects for an organism. The risk that a pharmacological interaction will appear increases as a function of the number of drugs administered to a patient at the same time. Over a third (36%) of older adults in the U.S. regularly use 5 or more medications or supplements and 15% are potentially at risk for a major drug-drug interaction.[4] Both the use of medications and subsequent adverse drug interactions have increased significantly between 2005-2011.[4]
It is possible that an interaction will occur between a drug and another substance present in the organism (i.e. foods or alcohol). Or in certain specific situations a drug may even react with itself, such as occurs with dehydration. In other situations, the interaction does not involve any effect on the drug. In certain cases, the presence of a drug in an individual's blood may affect certain types of laboratory analysis (analytical interference).
It is also possible for interactions to occur outside an organism before administration of the drugs has taken place. This can occur when two drugs are mixed, for example, in a saline solution prior to intravenous injection. Some classic examples of this type of interaction include that Thiopentone and Suxamethonium should not be placed in the same syringe and same is true for Benzylpenicillin and Heparin. These situations will all be discussed under the same heading due to their conceptual similarity.
Drug interactions may be the result of various processes. These processes may include alterations in the pharmacokinetics of the drug, such as alterations in the absorption, distribution, metabolism, and excretion (ADME) of a drug. Alternatively, drug interactions may be the result of the pharmacodynamic properties of the drug, e.g. the co-administration of a receptor antagonist and an agonist for the same receptor.
Synergy and antagonism
When the interaction causes an increase in the effects of one or both of the drugs the interaction is called a synergistic effect. An "additive synergy" occurs when the final effect is equal to the sum of the effects of the two drugs (Although some authors argue that this is not true synergy). When the final effect is much greater than the sum of the two effects this is called enhanced synergy. This concept is recognized by the majority of authors,[5] although other authors only refer to synergy when there is an enhanced effect. These authors use the term "additive effect" for additive synergy and they reserve use of the term "synergistic effect" for enhanced synergy.[6] The opposite effect to synergy is termed antagonism. Two drugs are antagonistic when their interaction causes a decrease in the effects of one or both of the drugs.
Both synergy and antagonism can both occur during different phases of the interaction of a drug with an organism, with each effect having a different name. For example, when the synergy occurs at a cellular receptor level this is termed agonism, and the substances involved are termed agonists. On the other hand, in the case of antagonism the substances involved are known as inverse agonists. The different responses of a receptor to the action of a drug has resulted in a number of classifications, which use terms such as "partial agonist", "competitive agonist" etc. These concepts have fundamental applications in the pharmacodynamics of these interactions. The proliferation of existing classifications at this level, along with the fact that the exact reaction mechanisms for many drugs are not well understood means that it is almost impossible to offer a clear classification for these concepts. It is even likely that many authors would misapply any given classification.[5]
Underlying factors
It is possible to take advantage of positive drug interactions. However, the negative interactions are usually of more interest because of their pathological significance and also because they are often unexpected and may even go undiagnosed. By studying the conditions that favour the appearance of interactions it should be possible to prevent them or at least diagnose them in time. The factors or conditions that predispose or favour the appearance of interactions include:[5]
- Old age: factors relating to how human physiology changes with age may affect the interaction of drugs. For example, liver metabolism, kidney function, nerve transmission or the functioning of bone marrow all decrease with age. In addition, in old age there is a sensory decrease that increases the chances of errors being made in the administration of drugs.[7]
- Polypharmacy: The more drugs a patient takes the more likely it will be that some of them will interact.[8]
- Genetic factors: Genes synthesize enzymes that metabolize drugs. Some races have genotypic variations that could decrease or increase the activity of these enzymes. The consequence of this would, on occasions, be a greater predisposition towards drug interactions and therefore a greater predisposition for adverse effects to occur. This is seen in genotype variations in the isozymes of cytochrome P450.
- Hepatic or renal diseases: The blood concentrations of drugs that are metabolized in the liver and / or eliminated by the kidneys may be altered if either of these organs is not functioning correctly. If this is the case an increase in blood concentration is normally seen.[8]
- Serious diseases that could worsen if the dose of the medicine is reduced.
- Drug dependent factors:[9]
- Narrow therapeutic index: Where the difference between the effective dose and the toxic dose is small.[n. 1] The drug digoxin is an example of this type of drug.
- Steep dose-response curve: Small changes in the dosage of a drug produce large changes in the drug's concentration in the patient's blood plasma.
- Saturable hepatic metabolism: In addition to dose effects the capacity to metabolize the drug is greatly decreased
Analytical interference
The detection of laboratory parameters is based on physicochemical reactions between the substance being measured and reagents designed for this purpose. These reactions can be altered by the presence of drugs giving rise to an over estimation or an underestimation of the real results. Levels of cholesterol and other blood lipids can be overestimated as a consequence of the presence in the blood of some psychotropic drugs. These overestimates should not be confused with the action of other drugs that actually increase blood cholesterol levels due to an interaction with its metabolism. Most experts consider that these are not true interactions, so they will not be dealt with further in this discussion.[10]
These chemical reactions are also known as pharmacological incompatibilities. The reactions occur when two or more drugs are mixed outside the body of the organism for the purpose of joint administration.[3] Usually the interaction is antagonistic and it almost always affects both drugs. Examples of these types of interactions include the mixing of penicillins and aminoglycosides in the same serum bottle, which causes the formation of an insoluble precipitate, or the mixing of ciprofloxacin with furosemide. The interaction of some drugs with the transport medium can also be included here. This means that certain drugs cannot be administered in plastic bottles because they bind with the bottle's walls, reducing the drug's concentration in solution.
Many authors do not consider them to be interactions in the strictest sense of the word. An example is the database of the General Council of Official Pharmacists Colleges of Spain (Consejo General de Colegios Oficiales de Farmacéuticos de España),[11] that does not include them among the 90,000 registered interactions.
Pharmacodynamic interactions
The change in an organism's response on administration of a drug is an important factor in pharmacodynamic interactions. These changes are extraordinarily difficult to classify given the wide variety of modes of action that exist and the fact that many drugs can cause their effect through a number of different mechanisms. This wide diversity also means that, in all but the most obvious cases, it is important to investigate and understand these mechanisms. The well-founded suspicion exists that there are more unknown interactions than known ones.
Pharmacodynamic interactions can occur on:
- Pharmacological receptors:[12] Receptor interactions are the most easily defined, but they are also the most common. From a pharmacodynamic perspective, two drugs can be considered to be:
- Homodynamic, if they act on the same receptor. They, in turn can be:
- Pure agonists, if they bind to the main locus of the receptor, causing a similar effect to that of the main drug.
- Partial agonists if, on binding to one of the receptor's secondary loci, they have the same effect as the main drug, but with a lower intensity.
- Antagonists, if they bind directly to the receptor's main locus but their effect is opposite to that of the main drug. These include:
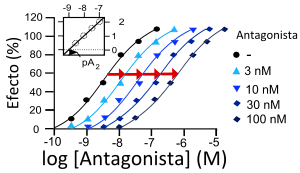
- Competitive antagonists, if they compete with the main drug to bind with the receptor. The amount of antagonist or main drug that binds with the receptor will depend on the concentrations of each one in the plasma.
- Uncompetitive antagonists, when the antagonist binds to the receptor irreversibly and is not released until the receptor is saturated. In principle the quantity of antagonist and agonist that binds to the receptor will depend on their concentrations. However, the presence of the antagonist will cause the main drug to be released from the receptor regardless of the main drug's concentration, therefore all the receptors will eventually become occupied by the antagonist.
- Heterodynamic competitors, if they act on distinct receptors.
- Homodynamic, if they act on the same receptor. They, in turn can be:
- Signal transduction mechanisms: these are molecular processes that commence after the interaction of the drug with the receptor.[13] For example, it is known that hypoglycaemia (low blood glucose) in an organism produces a release of catecholamines, which trigger compensation mechanisms thereby increasing blood glucose levels. The release of catecholamines also triggers a series of symptoms, which allows the organism to recognise what is happening and which act as a stimulant for preventative action (eating sugars). Should a patient be taking a drug such as insulin, which reduces glycaemia, and also be taking another drug such as certain beta-blockers for heart disease, then the beta-blockers will act to block the adrenaline receptors. This will block the reaction triggered by the catecholamines should a hypoglycaemic episode occur. Therefore, the body will not adopt corrective mechanisms and there will be an increased risk of a serious reaction resulting from the ingestion of both drugs at the same time.
- Antagonic physiological systems:[13] Imagine a drug A that acts on a certain organ. This effect will increase with increasing concentrations of physiological substance S in the organism. Now imagine a drug B that acts on another organ, which increases the amount of substance S. If both drugs are taken simultaneously it is possible that drug A could cause an adverse reaction in the organism as its effect will be indirectly increased by the action of drug B. An actual example of this interaction is found in the concomitant use of digoxin and furosemide. The former acts on cardiac fibres and its effect is increased if there are low levels of potassium (K) in blood plasma. Furosemide is a diuretic that lowers arterial tension but favours the loss of K+. This could lead to hypopotassaemia (low levels of potassium in the blood), which could increase the toxicity of digoxin.
Pharmacokinetic interactions
Modifications in the effect of a drug are caused by differences in the absorption, transport, distribution, metabolization or excretion of one or both of the drugs compared with the expected behaviour of each drug when taken individually. These changes are basically modifications in the concentration of the drugs. In this respect two drugs can be homergic if they have the same effect in the organism and heterergic if their effects are different.
Absorption interactions
Changes in motility
Some drugs, such as the prokinetic agents increase the speed with which a substance passes through the intestines. If a drug is present in the digestive tract’s absorption zone for less time its blood concentration will decrease. The opposite will occur with drugs that decrease intestinal motility.
- pH: Drugs can be present in either ionised or non-ionised form, depending on their pKa (pH at which the drug reaches equilibrium between its ionised and non-ionised form).[14] The non-ionized forms of drugs are usually easier to absorb, because they will not be repelled by the lipidic bylayer of the cell, most of them can be absorbed by passive diffusion, unless they are too big or too polarized (like glucose or vancomicyn), in which case they may have or not specific and non specific transporters distributed on the entire intestine internal surface, that carries drugs inside the body. Obviously increasing the absorption of a drug will increase its bioavailability, so, changing the drug's state between ionized or not, can be useful or not for certain drugs.
Certain drugs require an acid stomach pH for absorption. Others require the basic pH of the intestines. Any modification in the pH could change this absorption. In the case of the antacids, an increase in pH can inhibit the absorption of other drugs such as zalcitabine (absorption can be decreased by 25%), tipranavir (25%) and amprenavir (up to 35%). However, this occurs less often than an increase in pH causes an increase in absorption. Such as occurs when cimetidine is taken with didanosine. In this case a gap of two to four hours between taking the two drugs is usually sufficient to avoid the interaction.[15]
- Drug solubility: The absorption of some drugs can be drastically reduced if they are administered together with food with a high fat content. This is the case for oral anticoagulants and avocado.
- Formation of non-absorbable complexes:
- Chelation: The presence of di- or trivalent cations can cause the chelation of certain drugs, making them harder to absorb. This interaction frequently occurs between drugs such as tetracycline or the fluoroquinolones and dairy products (due to the presence of Ca++).
- Binding with proteins. Some drugs such as sucralfate binds to proteins, especially if they have a high bioavailability. For this reason its administration is contraindicated in enteral feeding.[16]
- Finally, another possibility is that the drug is retained in the intestinal lumen forming large complexes that impede its absorption. This can occur with cholestyramine if it is associated with sulfamethoxazol, thyroxine, warfarin or digoxin.
- Acting on the P-glycoprotein of the enterocytes: This appears to be one of the mechanisms promoted by the consumption of grapefruit juice in increasing the bioavailability of various drugs, regardless of its demonstrated inhibitory activity on first pass metabolism.[17]
Transport and distribution interactions
The main interaction mechanism is competition for plasma protein transport. In these cases the drug that arrives first binds with the plasma protein, leaving the other drug dissolved in the plasma, which modifies its concentration. The organism has mechanisms to counteract these situations (by, for example, increasing plasma clearance), which means that they are not usually clinically relevant. However, these situations should be taken into account if there other associated problems are present such as when the method of excretion is affected.[18]
Metabolism interactions

Many drug interactions are due to alterations in drug metabolism.[19] Further, human drug-metabolizing enzymes are typically activated through the engagement of nuclear receptors.[19] One notable system involved in metabolic drug interactions is the enzyme system comprising the cytochrome P450 oxidases.
CYP450
Cytochrome P450 is a very large family of haemoproteins (hemoproteins) that are characterized by their enzymatic activity and their role in the metabolism of a large number of drugs.[20] Of the various families that are present in human beings the most interesting in this respect are the 1, 2 and 3, and the most important enzymes are CYP1A2, CYP2C9, CYP2C19, CYP2D6, CYP2E1 and CYP3A4.[21] The majority of the enzymes are also involved in the metabolism of endogenous substances, such as steroids or sex hormones, which is also important should there be interference with these substances. As a result of these interactions the function of the enzymes can either be stimulated (enzyme induction) or inhibited (enzyme inhibition).
Enzymatic inhibition
If drug A is metabolized by a cytochrome P450 enzyme and drug B inhibits or decreases the enzyme's activity, then drug A will remain with high levels in the plasma for longer as its inactivation is slower. As a result, enzymatic inhibition will cause an increase in the drug's effect. This can cause a wide range of adverse reactions.
It is possible that this can occasionally lead to a paradoxical situation, where the enzymatic inhibition causes a decrease in the drug's effect: if the metabolism of drug A gives rise to product A2, which actually produces the effect of the drug. If the metabolism of drug A is inhibited by drug B the concentration of A2 that is present in the blood will decrease, as will the final effect of the drug.
Enzymatic induction
If drug A is metabolized by a cytochrome P450 enzyme and drug B induces or increases the enzyme's activity, then blood plasma concentrations of drug A will quickly fall as its inactivation will take place more rapidly. As a result, enzymatic induction will cause a decrease in the drug's effect.
As in the previous case it is possible to find paradoxical situations where an active metabolite causes the drug's effect. In this case the increase in active metabolite A2 (following the previous example) produces an increase in the drug's effect.
It can often occur that a patient is taking two drugs that are enzymatic inductors, one inductor and the other inhibitor or both inhibitors, which greatly complicates the control of an individual's medication and the avoidance of possible adverse reactions.
An example of this is shown in the following table for the CYP1A2 enzyme, which is the most common enzyme found in the human liver. The table shows the substrates (drugs metabolized by this enzyme) and the inductors and inhibitors of its activity:[21]
| Substrates. | Inhibitors. | Inductors. |
|---|---|---|
Enzyme CYP3A4 is the enzyme that the greatest number of drugs use as a substrate. Over 100 drugs depend on its metabolism for their activity and many others act on the enzyme as inductors or inhibitors.
Some foods also act as inductors or inhibitors of enzymatic activity. The following table shows the most common:
| Food. | Mechanism. | Drugs affected. |
|---|---|---|
| Enzymatic inductor | Acenocoumarol, warfarin | |
| Grapefruit juice | Enzymatic inhibition |
Main article: Grapefruit drug interactions |
| Soya | Enzymatic inhibition | Clozapine, Haloperidol, Olanzapine, caffeine, NSAIAs, Phenytoin, Zafirlukast, warfarin |
| Garlic | Increases antiplatelet activity | |
| Ginseng | To be determined | Warfarin, Heparin, Aspirin and NSAIA |
| Ginkgo biloba | Strong inhibitor of platelet aggregation factor | Warfarin, Aspirin and NSAIA |
| Hypericum perforatum (St John’s wort) | Enzymatic inductor (CYP450) | Warfarin, Digoxin, Theophylline, cyclosporine, phenytoin and antiretrovirals |
| Ephedra | Receptor level agonist | MAOI, central nervous system stimulants, alkaloids ergotamines and xanthines |
| Kava (Piper methysticum) | Unknown | Levodopa |
| Ginger | Inhibits thromboxane synthetase (in vitro) | Anticoagulants |
| Chamomile | Unknown | Benzodiazepines, barbiturates and opioid |
| Hawthorn | Unknown | Beta-adrenergic antagonists, Cisapride, Digoxin, Quinidine |
_white_bg.jpg)
Any study of pharmacological interactions between particular medicines should also discuss the likely interactions of some medicinal plants. The effects caused by medicinal plants should be considered in the same way as those of medicines as their interaction with the organism gives rise to a pharmacological response. Other drugs can modify this response and also the plants can give rise to changes in the effects of other active ingredients. There is little data available regarding interactions involving medicinal plants for the following reasons:

- False security regarding medicinal plants. The interaction between a medicinal plant and a drug is usually overlooked due to a believe in the "safety of medicinal plants"
- Variability of composition, both qualitative and quantitative. The composition of a plant-based drug is often subject to wide variations due to a number of factors such as seasonal differences in concentrations, soil type, climatic changes or the existence of different varieties or chemical races within the same plant species that have variable compositions of the active ingredient. On occasions an interaction can be due to just one active ingredient, but this can be absent in some chemical varieties or it can be present in low concentrations, which will not cause an interaction. Counter interactions can even occur. This occurs, for instance, with ginseng, the Panax ginseng variety increases the Prothrombin time, while the Panax quinquefolius variety decreases it.[24]
- Absence of use in at-risk groups, such as hospitalized and polypharmacy patients, who tend to have the majority of drug interactions.
- Limited consumption of medicinal plants has given rise to a lack of interest in this area.[25]
They are usually included in the category of foods as they are usually taken as a tea or food supplement. Although medicinal plants are increasingly being taken in a manner more usually associated with medicines: pills, tablets, capsules, etc.
Excretion interactions
Renal excretion

Only the free fraction of a drug that is dissolved in the blood plasma can be removed through the kidney. Therefore, drugs that are tightly bound to proteins are not available for renal excretion, as long as they are not metabolized when they may be eliminated as metabolites.[26] Creatinine clearance is used as a measure of kidney functioning but it is only useful in cases where the drug is excreted in an unaltered form in the urine. The excretion of drugs from the kidney's nephrons has the same properties as that of any other organic solute: passive filtration, reabsorption and active secretion. In the latter phase the secretion of drugs is an active process that is subject to conditions relating to the saturability of the transported molecule and competition between substrates. Therefore, these are key sites where interactions between drugs could occur. Filtration depends on a number of factors including the pH of the urine, it having been shown that the drugs that act as weak bases are increasingly excreted as the pH of the urine becomes more acidic, and the inverse is true for weak acids. This mechanism is of great use when treating intoxications (by making the urine more acidic or more alkali) and it is also used by some drugs and herbal products to produce their interactive effect.
| Weak acids | Weak bases |
|---|---|
Bile excretion
Bile excretion is different from kidney excretion as it is always involves energy expenditure in active transport across the epithelium of the bile duct against a concentration gradient. This transport system can also be saturated if the plasma concentrations of the drug are high. Bile excretion of drugs mainly takes place where their molecular weight is greater than 300 and they contain both polar and lipophilic groups. The glucuronidation of the drug in the kidney also facilitates bile excretion. Substances with similar physicochemical properties can block the receptor, which is important in assessing interactions. A drug excreted in the bile duct can occasionally be reabsorbed by the intestines (in the entero-hepatic circuit), which can also lead to interactions with other drugs.
Epidemiology
Among US adults older than 55, 4% are taking medication and or supplements that put them at risk of a major drug interaction.[28] Potential drug-drug interactions have increased over time[29] and are more common in the low educated elderly even after controlling for age, sex, place of residence, and comorbidity.[30]
See also
- Deprescribing
- Drug-Interactions.eu
- Cytochrome P450
- Classification of Pharmaco-Therapeutic Referrals
- Pharmacokinetics
- Pharmacodynamics
- Polypharmacy
- interactions can be checked online with interaction checkers: not alle interaction checkers give the same answers
Notes
- ↑ The term effective dose is generally understood to mean the minimum amount of a drug that is need to produce the required effect. The toxic dose is the minimum amount of a drug that will produce a damaging effect.
References
- ↑ " National Prescribing Service, 2009. Available at http://nps.org.au/news_and_media/media_releases/repository/Forget_the_colour_shape_or_brand__its
- ↑ "What really happens when you mix medications?". TED (talks). Retrieved April 2, 2016.
- 1 2 María Soledad Fernández Alfonso, Mariano Ruiz Gayo. Fundamentos de Farmacología Básica y Clínica. page 232. ISBN 84-8004-689-9
- 1 2 Qato DM; Wilder J; Schumm L; Gillet V; Alexander G (2016-04-01). "CHanges in prescription and over-the-counter medication and dietary supplement use among older adults in the united states, 2005 vs 2011". JAMA Internal Medicine. 176 (4): 473–482. doi:10.1001/jamainternmed.2015.8581. ISSN 2168-6106.
- 1 2 3 Baños Díez, J. E.; March Pujol, M (2002). Farmacología ocular (in Spanish) (2da ed.). Edicions UPC. p. 87. ISBN 8483016478. Retrieved 23 May 2009.
- ↑ Suárez Zuzunaga, A. Justificación Farmacológica para las Asociaciones Analgésicas Available on [www.spmed.org.pe/portal/images/stories/biliotecavirtual/.../dolor/justificacion_farmacolgica_para_las_asociaciones_analgesicas.ppt ]
- ↑ Merle L, Laroche ML, Dantoine T, Charmes JP (2005). "Predicting and Preventing Adverse Drug Reactions in the Very Old". Drugs and Aging. 22 (5): 375–392. doi:10.2165/00002512-200522050-00003.
- 1 2 García Morillo, J.S. Optimización del tratamiento de enfermos pluripatológicos en atención primaria UCAMI HHUU Virgen del Rocio. Sevilla. Spain. Available for members of SEMI at: ponencias de la II Reunión de Paciente Pluripatológico y Edad Avanzada
- ↑ Castells Molina,S.; Castells,S. y Hernández Pérez, M. Farmacología en enfermería Published by Elsevier Spain, 2007 ISBN 84-8174-993-1, 9788481749939 Available from
- ↑ Gago Bádenas, F. Curso de Farmacología General. Tema 7.- Interacciones farmacológicas. en
- ↑ Panorama Actual del Medicamento, number 245, July–August 2001, pages. 583–590
- ↑ S Gonzalez. "Interacciones Farmacológicas" (in Spanish). Retrieved 2009. Check date values in:
|access-date=(help) - 1 2 Curso de Farmacología Clínica Aplicada, in El Médico Interactivo
- ↑ Malgor — Valsecia, Farmacología general: Farmacocinética.Cap. 2. en Revised 25 September 2008
- ↑ Alicia Gutierrez Valanvia y Luis F. López-Cortés Interacciones farmacológicas entre fármacos antirretrovirales y fármacos usados para ciertos transtornos gastrointestinales. on accessed 24 September 2008
- 1 2 Marduga Sanz, Mariano. Interacciones de los alimentos con los medicamentos. on
- ↑ Tatro,DS. Update: Drug interaction with grapefruit juice. Druglink, 2004. 8 (5), page 35ss
- ↑ Valsecia, Mabel en
- 1 2 Elizabeth Lipp (2008-06-15). "Tackling Drug-Interaction Issues Early On". Genetic Engineering & Biotechnology News. Mary Ann Liebert, Inc. pp. 14, 16, 18, 20. Retrieved 2008-07-06.
(subtitle) Researchers explore a number of strategies to better predict drug responses in the clinic
- ↑ IUPAC, Compendium of Chemical Terminology, 2nd ed. (the "Gold Book") (1997). Online corrected version: (2006–) "cytochrome P450". Danielson, P (2002). "The cytochrome P450 superfamily: biochemistry, evolution and drug metabolism in humans". Curr Drug Metab. 3 (6): 561–97. doi:10.2174/1389200023337054. PMID 12369887.
- 1 2 Nelson D (2003). Cytochrome P450s in humans. Consulted 9 May 2005.
- ↑ Bailey DG, Malcolm J, Arnold O, Spence JD (August 1998). "Grapefruit juice-drug interactions". Br J Clin Pharmacol. 46 (2): 101–10. doi:10.1046/j.1365-2125.1998.00764.x. PMC 1873672
 . PMID 9723817.
. PMID 9723817.
Comment in: Mouly S, Paine MF (August 2001). "Effect of grapefruit juice on the disposition of omeprazole". Br J Clin Pharmacol. 52 (2): 216–7. doi:10.1111/j.1365-2125.1978.00999.pp.x. PMC 2014525. PMID 11488783. - ↑ Covarrubias-Gómez, A.; et al. (January–March 2005). "¿Qué se auto-administra su paciente?: Interacciones farmacológicas de la medicina herbal". Revista Mexicana de Anestesiología. 28 (1): 32–42.
- ↑ J. C. Tres Interacción entre fármacos y plantas medicinales. on
- ↑ Zaragozá F, Ladero M, Rabasco AM et al. Plantas Medicinales (Fitoterapia Práctica). Second Edition, 2001.
- ↑ Gago Bádenas, F. Curso de Farmacología General. Tema 6.- Excreción de los fármacos. en
- ↑ , Farmacología general: Farmacocinética.Cap. 2. en Revised 25 September 2008
- ↑ Qato DM, Alexander GC, Conti RM, Johnson M, Schumm P, Lindau ST (December 2008). "Use of prescription and over-the-counter medications and dietary supplements among older adults in the United States". JAMA. 300 (24): 2867–78. doi:10.1001/jama.2008.892. PMC 2702513. PMID 19109115.
- ↑ Haider SI, Johnell K, Thorslund M, Fastbom J (2007). "Trends in polypharmacy and potential drug-drug interactions across educational groups in elderly patients in Sweden for the period 1992–2002". International Journal of Clinical Pharmacology and Therapeutics. 45 (12): 643–653. doi:10.5414/cpp45643. PMID 18184532.
- ↑ Haider SI, Johnell K, Weitoft GR, Thorslund M, Fastbom J (2009). "The influence of educational level on polypharmacy and inappropriate drug use: a register-based study of more than 600,000 older people.". Journal of the American Geriatrics Society. 57 (1): 62–69. doi:10.1111/j.1532-5415.2008.02040.x. PMID 19054196.
Bibliography
MA Cos. Interacciones de fármacos y sus implicancias clínicas. In: Farmacología Humana. Chap. 10, pp. 165–176. (J. Flórez y col. Eds). Masson SA, Barcelona. 1997.
External links
- Drug Interactions: What You Should Know. U.S. Food and Drug Administration, Center for Drug Evaluation and Research
- On MedlinePlus there is information for non-professionals about drug interactions
- Medfacts Pocket Guide of Drug Interactions, Nephrology Pharmacy Associates
- Cytochrome P450 table maintained by the Indiana University School of Medicine
- Drugs.com Drug Interaction Checker
- EHealthme.com drug interactions checker based on 30 million reports from FDA and community
- 11.500 possible interactions of 5.000 substances
- Drug-Interactions.eu. Drug interactions tool for multiple and non-drug interactions. Data from over 2500 drug labels and 5000 trials, 10000 active ingredients (drugs, metabolites, herbal and not traditional medicine products, excipients, solvents, drugs of abuse, etc.), 11000 constants, 7000 AUC ratio values, 300 enzymes.