Cutaneous leishmaniasis
| Cutaneous leishmaniasis | |
|---|---|
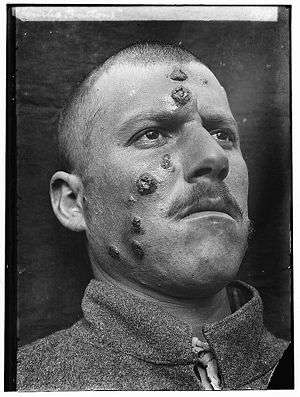 | |
| A man with cutaneous leishmaniasis in the Middle East, known then locally as "Jericho Buttons" for the frequency of cases near the ancient city of Jericho. | |
| Classification and external resources | |
| Specialty | infectious disease |
| ICD-10 | B55.1 |
| ICD-9-CM | 085.1-085.4 |
| DiseasesDB | 3266 29171 |
| MeSH | D016773 |
Cutaneous leishmaniasis (also known as oriental sore, tropical sore, chiclero ulcer, chiclero's ulcer or Aleppo boil)[1][2][3] is the most common form of leishmaniasis affecting humans.[4]:423 It is a skin infection caused by a single-celled parasite that is transmitted by the bite of a phlebotomine sandfly. There are about twenty species of Leishmania that may cause cutaneous leishmaniasis.
This disease is considered to be a zoonosis (an infectious disease that is naturally transmissible from vertebrate animals to humans), with the exception of Leishmania tropica — which is often an anthroponotic disease (an infectious disease that is naturally transmissible from humans to vertebrate animals).[3]
Signs and symptoms
Post kala-azar dermal leishmaniasis
Post-kala-azar dermal leishmaniasis (PKDL) is a recurrence of kala-azar that may appear on the skin of affected individuals months and up to 20 years after being partially treated, untreated or even in those considered adequately treated.[5][6] In Sudan, they can be demonstrated in up to 60% of treated cases. They manifest as hypopigmented skin lesions (such as macules, papules, nodules), or facial redness. Though any organism causing kala-azar can lead to PKDL, it is commonly associated with Leishmania donovani which gives different disease patterns in India and Sudan. In the Indian variant, nodules enlarge with time and form plaques but rarely ulcerate, but nodules from the African variety often ulcerate as they progress. Nerve involvement is common in African variety but rare in Indian subcontinent.[7] Histology demonstrates a mixture of chronic inflammatory cells; there can be macrophage or epitheloid granuloma.[8] Parasite concentration is not consistent among studies, perhaps reflecting low sensitivity of diagnostic methods used in earlier entries.
Current approach to diagnosis involves 1. demonstration of parasite by microscopy, in vitro culture or animal inoculation; 2. immunodiagnosis of parasite antigen; 3. detection of parasite DNA in tissue. Newer PCR based tools have higher sensitivity and specificity. Emergence of PKDL has been reported in HIV affected individuals [9] and may become a problem in future.
Sodium stibogluconate alone or in combination with rifampicin is used for the treatment of PKDL for a long course of up to 4 months. Compliance can be an issue for such a long course.
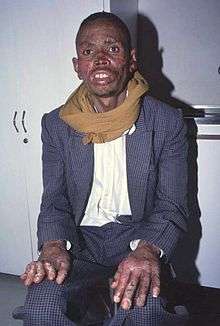
Mucocutaneous leishmaniasis
Mucocutaneous leishmaniasis is an especially disturbing form of cutaneous leishmaniasis, because it produces destructive and disfiguring lesions of the face. It is most often caused by Leishmania braziliensis, but cases caused by L. aethiopica have also been described.
Mucocutaneous leishmaniasis is very difficult to treat. Treatment involves the use of pentavalent antimonial compounds, which are highly toxic (common side effects include thrombophlebitis, pancreatitis, cardiotoxicity and hepatotoxicity) and not very effective. For example, in one study, despite treatment with high doses of sodium stibogluconate for 28 days, only 30% of patients remained disease-free at 12 months follow-up.[10] Even in those patients who achieve an apparent cure, as many as 19% will relapse.[11] Several drug combinations with immunomodulators have been tested, for example, a combination of pentoxifylline (inhibitor of TNF-α) and a pentavalent antimonial at a high dose for 30 days in a small-scale (23 patients) randomised placebo-controlled study from Brazil achieved cure rates of 90% and reduced time to cure,[12] a result that should be interpreted cautiously in light of inherent limitations of small-scale studies.[13] In an earlier small-scale (12 patients) study, addition of imiquimod showed promising results[14] which need yet to be confirmed in larger trials.
Pathophysiology

Promastigotes of Leishmania are transmitted to human skin by the bite of a sandfly. Leishmania then invades human macrophages and replicates intracellularly. A raised, red lesion develops at the site of the bite (often weeks or sometimes years afterwards). The lesion then ulcerates and may become secondarily infected with bacteria. In many species (for example, L. major) the lesion often spontaneously heals with atrophic scarring. In some species (for example, L. braziliensis) the lesion may spontaneously heal with scarring, but then reappear elsewhere (especially as destructive mucocutaneous lesions). Lesions of other Leishmania species may spontaneously heal and then reappear as satellite lesions around the site of the original lesion, or along the route of lymphatic drainage.
Some species tend to cause cutaneous leishmaniasis (e.g., L. major and L.tropica), whereas some species tend to cause visceral leishmaniasis (e.g., L. infantum and L. donovani), though emerging research (due to high deployment rates of western countries to indigenous areas) is showing these species specific presentation lines are blurring.
Diagnosis

Diagnosis is based on the characteristic appearance of non-healing raised, scaling lesions that may ulcerate and become secondarily infected with organisms such as Staphylococcus aureus, in someone who has returned from an endemic area.
The gold standard for diagnosis is PCR[15] (polymerase chain reaction) helps DNA polymerase to create new strands of DNA equivalent to template given.[16]
Treatment
The best treatment for cutaneous leishmaniasis is not known. Treatments that work for one species of leishmania may not work for another; it is recommended that advice of a tropical medicine or geographical medicine specialist be sought. Ideally, every effort should be made to establish the species of leishmania by molecular techniques (PCR) prior to starting treatment. In the setting of a developing country, there is often only one species present in a particular locality, so it is usually unnecessary to speciate every infection. Unfortunately, leishmaniasis is an orphan disease in developed nations, and almost all the current treatment options are toxic with significant side effects. The most sound treatment for cutaneous leishmaniasis thus far is prevention.
- Leishmania major :L. major infections are usually considered to heal spontaneously and do not require treatment, but there have been several reports of severe cases caused by L. major in Afghanistan. In Saudi Arabia, a six-week course of oral fluconazole 200 mg daily has been reported to speed up healing.[17] In a randomized clinical trial from Iran, fluconazole 400 mg daily was shown to be significantly more effective than fluconazole 200 mg daily in the treatment of cutaneous leishmaniasis.[18]
- Leishmania braziliensis :Treatment with pentavalent antimonials or amphotericin is necessary, because of the risk of developing disfiguring mucocutaneous lesions.
- Leishmania infantum :L. infantum causes cutaneous leishmaniasis in southern France.[19]
New treatment options are arising from the new oral drug miltefosine (Impavido) which has shown in several clinical trials to be very efficient and safe in visceral and cutaneous leishmaniasis. Recent studies from Bolivia show a high cure rate for mucocutaneous leishmaniasis. Comparative studies against pentavalent antimonials in Iran and Pakistan are also beginning to show a high cure rate for L. major and L. tropica. It is registered in many countries of Latin America, as well in Germany. In October 2006 it received orphan drug status from the US Food and Drug administration. The drug is generally better tolerated than other drugs. Main side effects are gastrointestinal disturbances in the 1–2 days of treatment which does not affect the efficacy.
Secondary bacterial infection (especially with Staphylococcus aureus) is common and may require antibiotics. Clinicians who are unfamiliar with cutaneous leishmaniasis may mistake the lesion for a pure bacterial infection (especially after isolation of S. aureus from bacterial skin swabs) and fail to consider the possibility of leishmaniasis.
Epidemiology

Cutaneous leishmaniasis is endemic in all tropical and subtropical areas of the world.[20] The distribution of this disease is very tightly linked to geography, and villages even 15 miles apart can have very different rates of cutaneous leishmaniasis.
Most species of Leishmania are capable of infecting humans and causing cutaneous leishmaniasis. In the New World, these organisms include L. amazonensis, L. braziliensis, L. guyanensis, L. lainsoni, L. lindenbergi, L. mexicana, L. naiffi, L. panamensis, L. peruviana, L. shawi, and L. venezuelensis. Old World species that cause cutaneous leishmaniasis include L. aethiopica, L. infantum, L. major, and L. tropica. With the exception of L. tropica — which is commonly associated with human settlements and therefore considered to be an anthroponotic species — all of these organisms are zoonotic.[3] As demographic changes occur in developing nations, some species that have traditionally been considered to be zoonotic (e.g., L. panamensis) are becoming primarily human pathogens.[21]
Dogs and rodents serve as the primary animal reservoir hosts in the sylvatic cycle, but people with chronic PKDL can also serve as important reservoir hosts for cutaneous leishmaniasis.[22] The most common vectors for cutaneous leishmaniasis in the Old World are sandflies of the genus Phlebotomus, while Lutzomyia and those within the family Psychodidae (especially the genus Psychodopygus) are the most common vectors in the New World. There are more than 600 species of phlebotomine sandflies, and only 30 of these are known vectors.[23] Cutaneous leishmaniasis has been seen in American and Canadian troops coming back from Afghanistan.[24]
Outbreak in 2016
The Middle East, in 2016, seems to be experiencing an increase in the cutaneous leishmaniasis disease due to migrants fleeing the Islamic State. Reports of the increase in the disease have surfaced in Turkey, Lebanon, and elsewhere.[25][26][27]
The huge increase in the spread of the disease is attributed to the refugee crises in the Middle East and North Africa over the past five years, particularly due to the displacement of millions of Syrian refugees.[28] The outbreak among Syrian refugees was documented by the World Health Organisation (WHO) in 2012 and recognised as ongoing.[29]
Other animals

Besides humans, cutaneous leishmaniasis often affects other animals, notably in dogs as canine leishmaniasis.[3]
References
- ↑ Calvopiña, M; Martinez, L; Hashiguchi, Y (2013). "Cutaneous leishmaniasis "chiclero's ulcer" in subtropical Ecuador". American Journal of Tropical Medicine and Hygiene. 89 (2): 195–6. doi:10.4269/ajtmh.12-0690. PMC 3741233
 . PMID 23926136.
. PMID 23926136. - ↑ Stowers, J.H. (1920). "Case of Delhi Boil or Sore (Syn.: Oriental Sore; Aleppo Boil)". Proceedings of the Royal Society for Medicine. 13 (Dermatol Sect): 81–83. PMC 2152205. PMID 19980989.
- 1 2 3 4 The Institute for International Cooperation in Animal Biologics and the Center for Food Security and Public Health (October 2009). "Leishmaniasis (cutaneous and visceral)" (PDF). Ames, Iowa: College of Veterinary Medicine, Iowa State University. Retrieved 2015-01-04.
- ↑ James, William D.; Berger, Timothy G. (2006). Andrews' Diseases of the Skin: clinical Dermatology. Saunders Elsevier. ISBN 978-0-7216-2921-6.
- ↑ Banerjee N (1973). "Role of I.M.A. during natural calamities and national emergencies". Journal of the Indian Medical Association. 61 (11): 477–81. PMID 4600129.
- ↑ Rathi SK, Pandhi RK, Chopra P, Khanna N; Pandhi; Chopra; Khanna (2005). "Post-kala-azar dermal leishmaniasis: a histopathological study". Indian journal of dermatology, venereology and leprology. 71 (4): 250–3. doi:10.4103/0378-6323.16616. PMID 16394433.
- ↑ Salotra P, Singh R; Singh (2006). "Challenges in the diagnosis of post-kala-azar dermal leishmaniasis". Indian J. Med. Res. 123 (3): 295–310. PMID 16778312.
- ↑ Singh N, Ramesh V, Arora VK, Bhatia A, Kubba A, Ramam M; Ramesh; Arora; Bhatia; Kubba; Ramam (1998). "Nodular post-kala-azar dermal leishmaniasis: a distinct histopathological entity". J Cutan Pathol. 25 (2): 95–9. doi:10.1111/j.1600-0560.1998.tb01696.x. PMID 9521498.
- ↑ Stark D, Pett S, Marriott D, Harkness J; Pett; Marriott; Harkness (2006). "Post-kala-azar dermal leishmaniasis due to Leishmania infantum in a human immunodeficiency virus type 1-infected patient". J Clin Microbiol. 44 (3): 1178–80. doi:10.1128/JCM.44.3.1178-1180.2006. PMC 1393159. PMID 16517925.
- ↑ Franke ED, Wignall FS, Cruz ME, et al. (1990). "Efficacy and toxicity of sodium stibogluconate for mucosal leishmaniasis". Ann Intern Med. 113 (12): 934–40. doi:10.7326/0003-4819-113-12-934. PMID 2173461.
- ↑ Netto EM, Marsden PD, Llanos-Cuentas EA, et al. (1990). "Long-term follow-up of patients with Leishmania (Viannia) braziliensis infection and treated with glucantime". Trans R Soc Trop Med Hyg. 84 (3): 367–70. doi:10.1016/0035-9203(90)90321-5. PMID 2260171.
- ↑ Machado PR, Lessa H, Lessa M, et al. (2007). "Oral pentoxifylline combined with pentavalent antimony: A randomized trial for mucosal leishmaniasis". Clin Infect Dis. 44 (6): 788–93. doi:10.1086/511643. PMID 17304449.
- ↑ Ojha, RP; Cervantes, D; Fischbach, LA (2007). "Oral pentoxifylline and pentavalent antimony for treatment of leishmaniasis: promising but inconclusive evidence of superiority, compared with antimony monotherapy". Clinical Infectious Diseases. 45 (8): 1104–6. doi:10.1086/521938. PMID 17879933.
- ↑ Arevalo I.; et al. (2001). "Successful treatment of drug-resistant cutaneous leishmaniasis in humans by use of imiquimod, an immunomodulator". Clin. Infect. Dis. 33 (11): 1847–51. doi:10.1086/324161. PMID 11692295.
- ↑ Reithinger R & Dujardin J-C; Dujardin (2007). "Molecular diagnosis of leishmaniasis: current status and future applications". J Clin Microbiol. 45 (1): 21–25. doi:10.1128/JCM.02029-06. PMC 1828971. PMID 17093038.
- ↑ "Polymerase Chain Reaction (PCR)". www.ncbi.nlm.nih.gov. Retrieved 2016-06-10.
- ↑ Alrajhi AA, Ibrahim EA, De Vol EB, et al. (2002). "Fluconazole for the treatment of cutaneous leishmaniasis caused by Leishmania major". N Engl J Med. 346 (12): 891–95. doi:10.1056/NEJMoa011882. PMID 11907288.
- ↑ Emad M, Hayati F, Fallahzadeh MK, Namazi MR (Mar 2011). "Superior efficacy of oral fluconazole 400 mg daily versus oral fluconazole 200 mg daily in the treatment of cutaneous leishmania major infection: a randomized clinical trial". Journal of the American Academy of Dermatology. 64 (3): 606–8. doi:10.1016/j.jaad.2010.04.014.
- ↑ Pratlong F.; et al. (2004). "Isoenzymatic analysis of 712 strains of Leishmania infantum in the south of France and relationship of enzymatic polymorphism to clinical and epidemiological features". Journal of Clinical Microbiology. 42 (9): 4077–82. doi:10.1128/jcm.42.9.4077-4082.2004. PMC 516332. PMID 15364993.
- 1 2 Aoun, K.; Bouratbine, A. (2014). "Cutaneous Leishmaniasis in North Africa: a review". Parasite. 21: 14. doi:10.1051/parasite/2014014. PMC 3952656. PMID 24626301.

- ↑ Vergel C, Palacios R, Cadena H, et al. (2006). "Evidence for Leishmania parasites in the skin and blood of patients before and after treatment". J Infect Dis. 194 (4): 503–511. doi:10.1086/505583. PMID 16845635.
- ↑ Centers for Disease Control and Prevention (July 10, 2014). "Parasites - leishmaniasis". Resources for health professionals. Atlanta, Georgia: United States Department of Health and Human Services. Retrieved 2015-01-04.
- ↑ Connolly, M. A.; Organization, World Health (2005). Communicable disease control in emergencies: a field manual. World Health Organization. pp. 152–. ISBN 978-92-4-154616-4. Retrieved 12 June 2016.
- ↑ "Canadian soldiers bring back Old World disease".
- ↑ "A disfiguring tropical disease is sweeping across the Middle East". The Independent. 30 May 2016. Retrieved 12 June 2016.
- ↑ "Graphic Pics: Migrants Fleeing Islamic State Risk Bringing Deadly Flesh Eating Disease To Europe". Breitbart. 30 May 2016. Retrieved 10 June 2016.
- ↑ Hiddleston, Sarah. "An old disease rears its ugly head". Nature Middle East. doi:10.1038/nmiddleeast.2016.82.
- ↑ PLoS article
- ↑ Ongoing epidemic