Fructose
| |||
 Haworth projection of β-D-Fructofuranose | |||
 Ball-and-stick model of D-fructose | |||
| Names | |||
|---|---|---|---|
| IUPAC name
1,3,4,5,6-Pentahydroxy-2-hexanone | |||
| Systematic IUPAC name
1,3,4,5,6-Pentahydroxy-2-hexanone | |||
| Other names | |||
| Identifiers | |||
| 57-48-7 | |||
| 3D model (Jmol) | Interactive image | ||
| ChEBI | CHEBI:28645 | ||
| ChEMBL | ChEMBL604608 | ||
| ChemSpider | 388775 | ||
| ECHA InfoCard | 100.000.303 | ||
| EC Number | 200-333-3 | ||
| KEGG | C02336 | ||
| PubChem | 5984 | ||
| UNII | 6YSS42VSEV | ||
| |||
| |||
| Properties | |||
| C6H12O6 | |||
| Molar mass | 180.16 g·mol−1 | ||
| Density | 1.694 g/cm3 | ||
| Melting point | 103 °C (217 °F; 376 K) | ||
| Pharmacology | |||
| V06DC02 (WHO) | |||
| Hazards | |||
| Lethal dose or concentration (LD, LC): | |||
| LD50 (median dose) |
15000 mg/kg (intravenous, rabbit)[3] | ||
| Except where otherwise noted, data are given for materials in their standard state (at 25 °C [77 °F], 100 kPa). | |||
| | |||
| Infobox references | |||


Fructose, or fruit sugar, is a simple ketonic monosaccharide found in many plants, where it is often bonded to glucose to form the disaccharide sucrose. It is one of the three dietary monosaccharides, along with glucose and galactose, that are absorbed directly into the bloodstream during digestion. Fructose was discovered by French chemist Augustin-Pierre Dubrunfaut in 1847.[4][5] The name "fructose" was coined in 1857 by the English chemist William Miller.[6] Pure, dry fructose is a very sweet, white, odorless, crystalline solid and is the most water-soluble of all the sugars.[7] Fructose is found in honey, tree and vine fruits, flowers, berries, and most root vegetables.
Commercially, fructose is frequently derived from sugar cane, sugar beets, and corn. Crystalline fructose is the monosaccharide, dried, ground, and of high purity. High fructose corn syrup (HFCS) is a mixture of glucose and fructose as monosaccharides. Sucrose is a compound with one molecule of glucose covalently linked to one molecule of fructose. All forms of fructose, including fruits and juices, are commonly added to foods and drinks for palatability and taste enhancement, and for browning of some foods, such as baked goods.
About 240,000 tonnes of crystalline fructose are produced annually.[8]
There are speculations that excessive fructose consumption is a cause of insulin resistance, obesity,[9] elevated LDL cholesterol and triglycerides, leading to metabolic syndrome,[10][11][12] type 2 diabetes and cardiovascular disease.[13] However, the European Food Safety Authority stated that fructose is preferred over sucrose and glucose in sugar-sweetened foods and beverages because of its lower effect on postprandial blood sugar levels.[14] Further, the UK's Scientific Advisory Committee on Nutrition in 2015 disputed the claims of fructose causing metabolic disorders, stating that "there is insufficient evidence to demonstrate that fructose intake ... leads to adverse health outcomes independent of any effects related to its presence as a component of total and free sugars."[15]
Chemical properties


Fructose is a 6-carbon polyhydroxyketone. Crystalline fructose adopts a cyclic six-membered structure owing to the stability of its hemiketal and internal hydrogen-bonding. This form is formally called D-fructopyranose. In solution, fructose exists as an equilibrium mixture of 70% fructopyranose and about 22% fructofuranose, as well as small amounts of three other forms, including the acyclic structure.[16]
Reactions
Fructose and fermentation
Fructose may be anaerobically fermented by yeast or bacteria.[17] Yeast enzymes convert sugar (glucose, or fructose) to ethanol and carbon dioxide. The carbon dioxide released during fermentation will remain dissolved in water, where it will reach equilibrium with carbonic acid, unless the fermentation chamber is left open to the air. The dissolved carbon dioxide and carbonic acid produce the carbonation in bottled fermented beverages.[18]
Fructose and Maillard reaction
Fructose undergoes the Maillard reaction, non-enzymatic browning, with amino acids. Because fructose exists to a greater extent in the open-chain form than does glucose, the initial stages of the Maillard reaction occur more rapidly than with glucose. Therefore, fructose has potential to contribute to changes in food palatability, as well as other nutritional effects, such as excessive browning, volume and tenderness reduction during cake preparation, and formation of mutagenic compounds.[19]
Dehydration
Fructose readily dehydrates to give hydroxymethylfurfural ("HMF"). This process, in the future, may become part of a low-cost, carbon-neutral system to produce replacements for petrol and diesel from plants.[20]
Physical and functional properties
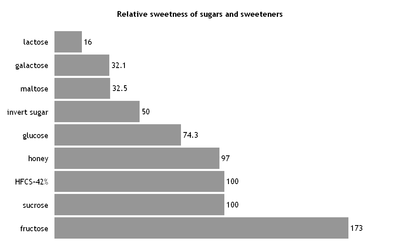
Sweetness of fructose
The primary reason that fructose is used commercially in foods and beverages, besides its low cost, is its high relative sweetness. It is the sweetest of all naturally occurring carbohydrates. In general, fructose is regarded as being 1.73 times as sweet as sucrose.[21][22] However, it is the 6-membered ring form of fructose that is sweeter; the 5-membered ring form tastes about the same as usual table sugar. Warming fructose leads to formation of the 5-membered ring form.[23]
The sweetness of fructose is perceived earlier than that of sucrose or glucose, and the taste sensation reaches a peak (higher than that of sucrose) and diminishes more quickly than that of sucrose. Fructose can also enhance other flavors in the system.[21]
Fructose exhibits a sweetness synergy effect when used in combination with other sweeteners. The relative sweetness of fructose blended with sucrose, aspartame, or saccharin is perceived to be greater than the sweetness calculated from individual components.[24]
Fructose solubility and crystallization
Fructose has higher solubility than other sugars as well as other sugar alcohols. Fructose is, therefore, difficult to crystallize from an aqueous solution.[21] Sugar mixes containing fructose, such as candies, are softer than those containing other sugars because of the greater solubility of fructose.[25]
Fructose hygroscopicity and humectancy
Fructose is quicker to absorb moisture and slower to release it to the environment than sucrose, glucose, or other nutritive sweeteners.[24] Fructose is an excellent humectant and retains moisture for a long period of time even at low relative humidity (RH). Therefore, fructose can contribute a more palatable texture, and longer shelf life to the food products in which it is used.[21]
Freezing point
Fructose has a greater effect on freezing point depression than disaccharides or oligosaccharides, which may protect the integrity of cell walls of fruit by reducing ice crystal formation. However, this characteristic may be undesirable in soft-serve or hard-frozen dairy desserts.[21]
Fructose and starch functionality in food systems
Fructose increases starch viscosity more rapidly and achieves a higher final viscosity than sucrose because fructose lowers the temperature required during gelatinizing of starch, causing a greater final viscosity.[26]
Although some artificial sweeteners are not suitable for home-baking, many traditional recipes use fructose.[27]
Food sources

Natural sources of fructose include fruits, vegetables (including sugar cane), and honey.[28] Fructose is often further concentrated from these sources. The highest dietary sources of fructose, besides pure crystalline fructose, are foods containing table sugar (sucrose), high-fructose corn syrup, agave nectar, honey, molasses, maple syrup, fruit and fruit juices, as these have the highest percentages of fructose (including fructose in sucrose) per serving compared to other common foods and ingredients. Fructose exists in foods either as a free monosaccharide or bound to glucose as sucrose, a disaccharide. Fructose, glucose, and sucrose may all be present in a food; however, different foods will have varying levels of each of these three sugars.
The sugar contents of common fruits and vegetables are presented in Table 1. In general, in foods that contain free fructose, the ratio of fructose to glucose is approximately 1:1; that is, foods with fructose usually contain about an equal amount of free glucose. A value that is above 1 indicates a higher proportion of fructose to glucose, and below 1 a lower proportion. Some fruits have larger proportions of fructose to glucose compared to others. For example, apples and pears contain more than twice as much free fructose as glucose, while for apricots the proportion is less than half as much fructose as glucose.
Apple and pear juices are of particular interest to pediatricians because the high concentrations of free fructose in these juices can cause diarrhea in children. The cells (enterocytes) that line children's small intestines have less affinity for fructose absorption than for glucose and sucrose.[29] Unabsorbed fructose creates higher osmolarity in the small intestine, which draws water into the gastrointestinal tract, resulting in osmotic diarrhea. This phenomenon is discussed in greater detail in the Health Effects section.
Table 1 also shows the amount of sucrose found in common fruits and vegetables. Sugarcane and sugar beet have a high concentration of sucrose, and are used for commercial preparation of pure sucrose. Extracted cane or beet juice is clarified, removing impurities; and concentrated by removing excess water. The end-product is 99.9%-pure sucrose. Sucrose-containing sugars include common table white granulated sugar and powdered sugar, as well as brown sugar.[30]
| Food Item | Total CarbohydrateA including "dietary fiber" |
Total Sugars |
Free Fructose |
Free Glucose |
Sucrose | Fructose/ Glucose Ratio |
Sucrose as a % of Total Sugars |
|---|---|---|---|---|---|---|---|
| Fruits | |||||||
| Apple | 13.8 | 10.4 | 5.9 | 2.4 | 2.1 | 2.0 | 19.9 |
| Apricot | 11.1 | 9.2 | 0.9 | 2.4 | 5.9 | 0.7 | 63.5 |
| Banana | 22.8 | 12.2 | 4.9 | 5.0 | 2.4 | 1.0 | 20.0 |
| Fig, dried | 63.9 | 47.9 | 22.9 | 24.8 | 0.9 | 0.93 | 0.15 |
| Grapes | 18.1 | 15.5 | 8.1 | 7.2 | 0.2 | 1.1 | 1 |
| Navel orange | 12.5 | 8.5 | 2.25 | 2.0 | 4.3 | 1.1 | 50.4 |
| Peach | 9.5 | 8.4 | 1.5 | 2.0 | 4.8 | 0.9 | 56.7 |
| Pear | 15.5 | 9.8 | 6.2 | 2.8 | 0.8 | 2.1 | 8.0 |
| Pineapple | 13.1 | 9.9 | 2.1 | 1.7 | 6.0 | 1.1 | 60.8 |
| Plum | 11.4 | 9.9 | 3.1 | 5.1 | 1.6 | 0.66 | 16.2 |
| Vegetables | |||||||
| Beet, Red | 9.6 | 6.8 | 0.1 | 0.1 | 6.5 | 1.0 | 96.2 |
| Carrot | 9.6 | 4.7 | 0.6 | 0.6 | 3.6 | 1.0 | 77 |
| Red Pepper, Sweet | 6.0 | 4.2 | 2.3 | 1.9 | 0.0 | 1.2 | 0.0 |
| Onion, Sweet | 7.6 | 5.0 | 2.0 | 2.3 | 0.7 | 0.9 | 14.3 |
| Sweet Potato | 20.1 | 4.2 | 0.7 | 1.0 | 2.5 | 0.9 | 60.3 |
| Yam | 27.9 | 0.5 | tr | tr | tr | na | tr |
| Sugar Cane | 13 – 18 | 0.2 – 1.0 | 0.2 – 1.0 | 11 – 16 | 1.0 | high | |
| Sugar Beet | 17 – 18 | 0.1 – 0.5 | 0.1 – 0.5 | 16 – 17 | 1.0 | high | |
| Grains | |||||||
| Corn, Sweet | 19.0 | 6.2 | 1.9 | 3.4 | 0.9 | 0.61 | 15.0 |
- ^A The carbohydrate figure is calculated in the USDA database and does not always correspond to the sum of the sugars, the starch, and the "dietary fiber".
All data with a unit of g (gram) are based on 100 g of a food item. The fructose/glucose ratio is calculated by dividing the sum of free fructose plus half sucrose by the sum of free glucose plus half sucrose.
Fructose is also found in the synthetically manufactured sweetener, high-fructose corn syrup (HFCS). Hydrolyzed corn starch is used as the raw material for production of HFCS. Through the enzymatic treatment, glucose molecules are converted into fructose.[30] There are three types of HFCS, each with a different proportion of fructose: HFCS-42, HFCS-55, and HFCS-90. The number for each HFCS corresponds to the percentage of synthesized fructose present in the syrup. HFCS-90 has the highest concentration of fructose, and typically, is used to manufacture HFCS-55; HFCS-55 is used as sweetener in soft drinks, whereas HFCS-42 is used in many processed foods and baked goods.
Carbohydrate content of commercial sweeteners (percent on dry basis)
| Sugar | Fructose | Glucose | Sucrose (Fructose+Glucose) |
Other sugars |
|---|---|---|---|---|
| Granulated sugar | 0 | 0 | 100 | 0 |
| Caramel | 1 | 1 | 97 | 1 |
| HFCS-42 | 42 | 53 | 0 | 5 |
| HFCS-55 | 55 | 41 | 0 | 4 |
| HFCS-90 | 90 | 5 | 0 | 5 |
| Honey | 50 | 44 | 1 | 5 |
| Maple syrup | 1 | 4 | 95 | 0 |
| Molasses | 23 | 21 | 53 | 3 |
| Tapioca Syrup | 55 | 45 | 0 | 0 |
| Corn syrup | 0 | 35 | 0 | 0 |
Data obtained from Kretchmer, N. & Hollenbeck, CB (1991). Sugars and Sweeteners, Boca Raton, FL: CRC Press, Inc.[30] for HFCS, and USDA for fruits and vegetables and the other refined sugars.[31]
Cane and beet sugars have been used as the major sweetener in food manufacturing for centuries. However, with the development of HFCS, a significant shift occurred in the type of sweetener consumption in certain countries, particularly the United States.[32] As seen in Figure 3, this change happened in the 1970s. Contrary to the popular belief, however, with the increase of HFCS consumption, the total fructose intake relative to the total glucose intake has not dramatically changed. Granulated sugar is 99.9%-pure sucrose, which means that it has equal ratio of fructose to glucose. The most commonly used forms of HFCS, HFCS-42, and HFCS-55 have a roughly equal ratio of fructose to glucose, with minor differences. HFCS has simply replaced sucrose as a sweetener. Therefore, despite the changes in the sweetener consumption, the ratio of glucose to fructose intake has remained relatively constant.[33]

Fructose digestion and absorption in humans

Fructose exists in foods either as a monosaccharide (free fructose) or as a unit of a disaccharide (sucrose). Free fructose is absorbed directly by the intestine. When fructose is consumed in the form of sucrose, it is digested (broken down) and then absorbed as free fructose. As sucrose comes into contact with the membrane of the small intestine, the enzyme sucrase catalyzes the cleavage of sucrose to yield one glucose unit and one fructose unit, which are then each absorbed. After absorption, it enters the hepatic portal vein and is directed toward the liver.
The mechanism of fructose absorption in the small intestine is not completely understood. Some evidence suggests active transport, because fructose uptake has been shown to occur against a concentration gradient.[34] However, the majority of research supports the claim that fructose absorption occurs on the mucosal membrane via facilitated transport involving GLUT5 transport proteins. Since the concentration of fructose is higher in the lumen, fructose is able to flow down a concentration gradient into the enterocytes, assisted by transport proteins. Fructose may be transported out of the enterocyte across the basolateral membrane by either GLUT2 or GLUT5, although the GLUT2 transporter has a greater capacity for transporting fructose, and, therefore, the majority of fructose is transported out of the enterocyte through GLUT2.
Capacity and rate of absorption
The absorption capacity for fructose in monosaccharide form ranges from less than 5 g to 50 g (per individual serving) and adapts with changes in dietary fructose intake.[35] Studies show the greatest absorption rate occurs when glucose and fructose are administered in equal quantities.[35] When fructose is ingested as part of the disaccharide sucrose, absorption capacity is much higher because fructose exists in a 1:1 ratio with glucose. It appears that the GLUT5 transfer rate may be saturated at low levels, and absorption is increased through joint absorption with glucose.[36] One proposed mechanism for this phenomenon is a glucose-dependent cotransport of fructose. In addition, fructose transfer activity increases with dietary fructose intake. The presence of fructose in the lumen causes increased mRNA transcription of GLUT5, leading to increased transport proteins. High-fructose diets (>2.4 g/kg body wt) increase transport proteins within three days of intake.[37]
Malabsorption
Several studies have measured the intestinal absorption of fructose using the hydrogen breath test.[38][39][40][41] These studies indicate that fructose is not completely absorbed in the small intestine. When fructose is not absorbed in the small intestine, it is transported into the large intestine, where it is fermented by the colonic flora. Hydrogen is produced during the fermentation process and dissolves into the blood of the portal vein. This hydrogen is transported to the lungs, where it is exchanged across the lungs and is measurable by the hydrogen breath test. The colonic flora also produces carbon dioxide, short-chain fatty acids, organic acids, and trace gases in the presence of unabsorbed fructose.[42] The presence of gases and organic acids in the large intestine causes gastrointestinal symptoms such as bloating, diarrhea, flatulence, and gastrointestial pain[38] Exercise immediately after consumption can exacerbate these symptoms by decreasing transit time in the small intestine, resulting in a greater amount of fructose emptied into the large intestine.[43]
Fructose metabolism
All three dietary monosaccharides are transported into the liver by the GLUT2 transporter.[44] Fructose and galactose are phosphorylated in the liver by fructokinase (Km= 0.5 mM) and galactokinase (Km = 0.8 mM). By contrast, glucose tends to pass through the liver (Km of hepatic glucokinase = 10 mM) and can be metabolised anywhere in the body. Uptake of fructose by the liver is not regulated by insulin. However, insulin is capable of increasing the abundance and functional activity of GLUT5 in skeletal muscle cells.[45]
Fructolysis
The initial catabolism of fructose is sometimes referred to as fructolysis, in analogy with glycolysis, the catabolism of glucose. In fructolysis, the enzyme fructokinase initially produces fructose 1-phosphate, which is split by aldolase B to produce the trioses dihydroxyacetone phosphate (DHAP) and glyceraldehyde . Unlike glycolysis, in fructolysis the triose glyceraldehyde lacks a phosphate group. A third enzyme, triokinase, is therefore required to phosphorylate glyceraldehyde, producing glyceraldehyde 3-phosphate. The resulting trioses are identical to those obtained in glycolysis and can enter the gluconeogenic pathway for glucose or glycogen synthesis, or be further catabolized through the lower glycolytic pathway to pyruvate.
Metabolism of fructose to DHAP and glyceraldehyde
The first step in the metabolism of fructose is the phosphorylation of fructose to fructose 1-phosphate by fructokinase, thus trapping fructose for metabolism in the liver. Fructose 1-phosphate then undergoes hydrolysis by aldolase B to form DHAP and glyceraldehydes; DHAP can either be isomerized to glyceraldehyde 3-phosphate by triosephosphate isomerase or undergo reduction to glycerol 3-phosphate by glycerol 3-phosphate dehydrogenase. The glyceraldehyde produced may also be converted to glyceraldehyde 3-phosphate by glyceraldehyde kinase or further converted to glycerol 3-phosphate by glycerol 3-phosphate dehydrogenase. The metabolism of fructose at this point yields intermediates in the gluconeogenic pathway leading to glycogen synthesis as well as fatty acid and triglyceride synthesis.
Synthesis of glycogen from DHAP and glyceraldehyde 3-phosphate
The resultant glyceraldehyde formed by aldolase B then undergoes phosphorylation to glyceraldehyde 3-phosphate. Increased concentrations of DHAP and glyceraldehyde 3-phosphate in the liver drive the gluconeogenic pathway toward glucose and subsequent glycogen synthesis.[46] It appears that fructose is a better substrate for glycogen synthesis than glucose and that glycogen replenishment takes precedence over triglyceride formation. Once liver glycogen is replenished, the intermediates of fructose metabolism are primarily directed toward triglyceride synthesis.

Synthesis of triglyceride from DHAP and glyceraldehyde 3-phosphate
Carbons from dietary fructose are found in both the free fatty acid and glycerol moieties of plasma triglycerides. High fructose consumption can lead to excess pyruvate production, causing a buildup of Krebs cycle intermediates.[47] Accumulated citrate can be transported from the mitochondria into the cytosol of hepatocytes, converted to acetyl CoA by citrate lyase and directed toward fatty acid synthesis.[47][48] In addition, DHAP can be converted to glycerol 3-phosphate, providing the glycerol backbone for the triglyceride molecule.[48] Triglycerides are incorporated into very-low-density lipoproteins (VLDL), which are released from the liver destined toward peripheral tissues for storage in both fat and muscle cells.

Fructose synthesis
Humans are capable of synthesizing fructose from glucose via the polyol pathway. This pathway is used by the seminal vesicles to secrete fructose into semen where it is a major source of energy for sperm.
Potential health effects
Digestion
Fructose absorption occurs in the small intestine via the GLUT-5[49] (fructose only) transporter, and the GLUT2 transporter, for which it competes with glucose and galactose. Over-consumption of fructose, inhibition of GLUT2 by other phytochemicals, such as flavonoids,[50] or other issues, may result in delivery of unabsorbed fructose into the large intestine, which will cause more water to be drawn into the large intestine through the process of osmosis causing diarrhea.[51] In addition, the excessive fructose becomes a source of nutrients for the gut flora resulting in a higher production of short chain fatty acids, hydrogen, carbon dioxide and other gases due to fermentation.[52] This increase of gas causes gastrointestinal side effects that mimic irritable bowel syndrome.[52]
Weight gain
In a meta-analysis of clinical trials with controlled feeding — where test subjects were fed a fixed amount of energy rather than being allowed to choose the amount they ate — fructose was not an independent factor for weight gain. In one study of a diet with excessive calories, fructose consumption was associated with weight gain.[53]
Cardiometabolic diseases
Excess fructose consumption has been hypothesized to be a cause of insulin resistance, obesity,[9][54] elevated LDL cholesterol and triglycerides, leading to metabolic syndrome.[10][54] In preliminary research, fructose consumption was correlated with obesity.[11][55] Fructose encourages visceral adipose tissue deposition in humans.[12][56]
Studies indicate that there may be an increased risk of cardiovascular disease from a high intake of fructose.[57] Studies have associated high fructose consumption with increased incidence of hypertension, both acutely [58] and in the long term in subjects without a history of hypertension.[59] The mechanistic link for this is thought to be the increased production of uric acid,[60] a known predictor for hypertension.[61] The elevation in uric acid is due to unregulated phosphorylation leading to depletion of ATP and subsequent ADP degradation to uric acid.[62]
Another study in humans concluded that fructose and sucrose are metabolized similarly,[63] whereas a different analysis "produced significantly higher fasting plasma triglyceride values than did the glucose diet in men" and "...if plasma triacylglycerols are a risk factor for cardiovascular disease, then diets high in fructose may be undesirable".[64] A study in 2015 later confirmed this by showing that consuming beverages with high levels of high fructose corn syrup caused heightened levels of LDL cholesterol, non-HDL cholesterol, apolipoprotein B, all of which are lipid/lipoproteins risk factors for cardiovascular disease.[65]
In contrast to the above claims of fructose contributing to cardiometabolic diseases, an expert panel of the European Food Safety Authority concluded that fructose be preferred in food and beverage manufacturing to replace sucrose and glucose due to the lower effect of fructose on blood glucose levels following a meal.[14]
Compared with sucrose
Fructose is often recommended for diabetics because it does not trigger the production of insulin by pancreatic β cells, probably because β cells have low levels of GLUT5,[66][67][68] although the net effect for both diabetics[69] and non-diabetics is debated. Fructose has a low glycemic index of 19 ± 2, compared with 100 for glucose and 68 ± 5 for sucrose.[70] Fructose is also 73% sweeter than sucrose at room temperature, so diabetics can use less of it. Studies show that fructose consumed before a meal may even lessen the glycemic response of the meal.[71] Fructose-sweetened food and beverage products cause less of a rise in blood glucose levels than do those manufactured with sucrose or glucose.[14]
Liver function
Excessive fructose consumption may contribute to the development of non-alcoholic fatty liver disease.[72][73]
Gout
A 2008 study found a risk of incident gout associated with high consumption of fructose or fructose-rich foods.[74]
Glycemic index
Fructose has the lowest glycemic index (GI = 19) of all the natural sugars. In comparison, ordinary table sugar (sucrose, which is half fructose) has a GI of 65 and honey (usually about 50% fructose content) has a GI of 55.
Appetite control
Compared with consumption of high glucose beverages, drinking high-fructose beverages with meals results in lower circulating insulin and leptin levels, and higher ghrelin levels after the meal.[75] Since leptin and insulin decrease appetite and ghrelin increases appetite, some researchers suspect that eating large amounts of fructose increases the likelihood of weight gain.[76]
See also
References
- ↑ "Fructose – Definition and More from the Free Merriam-Webster Dictionary". Mw4.m-w.com. Retrieved 10 December 2014.
- ↑ Levulose comes from the Latin word laevus, levo, "left side", levulose is the old word for the most occurring isomer of fructose. D-fructose rotate plane-polarised light to the left, hence the name..
- ↑ Michael Chambers. "ChemIDplus – 57-48-7 – BJHIKXHVCXFQLS-UYFOZJQFSA-N – Fructose [USP:JAN] – Similar structures search, synonyms, formulas, resource links, and other chemical information.". Chem.sis.nlm.nih.gov. Retrieved 10 December 2014.
- ↑ Dubrunfaut (1847) "Sur une propriété analytique des fermentations alcoolique et lactique, et sur leur application à l'étude des sucres" (On an analytic property of alcoholic and lactic fermentations, and on their application to the study of sugars), Annales de Chimie et de Physique, 21 : 169–178. On page 174, Dubrunfaut relates the discovery and properties of fructose.
- ↑ Fruton, J.S. Molecules of Life 1972, Wiley-Interscience
- ↑ William Allen Miller, Elements of Chemistry: Theoretical and Practical, Part III. Organic Chemistry (London, England: John W. Parker and son, 1857), pages 52 and 57.
- ↑ Hyvonen, L. & Koivistoinen, P (1982). "Fructose in Food Systems". In Birch, G.G. & Parker, K.J. Nutritive Sweeteners. London & New Jersey: Applied Science Publishers. pp. 133–144. ISBN 0-85334-997-5.
- ↑ Wolfgang Wach "Fructose" in Ullmann's Encyclopedia of Industrial Chemistry 2004, Wiley-VCH, Weinheim.doi:10.1002/14356007.a12_047.pub2
- 1 2 Elliott SS, Keim NL, Stern JS, Teff K, Havel PJ (2002). "Fructose, weight gain, and the insulin resistance syndrome". Am. J. Clin. Nutr. 76 (5): 911–22. PMID 12399260.
- 1 2 Basciano H, Federico L, Adeli K (2005). "Fructose, insulin resistance, and metabolic dyslipidemia". Nutrition & Metabolism. 2 (5): 5. doi:10.1186/1743-7075-2-5. PMC 552336
 . PMID 15723702.
. PMID 15723702. - 1 2 Isganaitis E; Lustig RH (2005). "Fast food, central nervous system insulin resistance, and obesity". Arterioscler. Thromb. Vasc. Biol. 25 (12): 2451–62. doi:10.1161/01.ATV.0000186208.06964.91. PMID 16166564.
- 1 2 Malik, Vasanti S.; Hu, Frank B. (2015). "Fructose and Cardiometabolic Health". Journal of the American College of Cardiology. 66 (14): 1615–1624. doi:10.1016/j.jacc.2015.08.025. ISSN 0735-1097. PMID 26429086.
- ↑ Rippe, James M.; Angelopoulos, Theodore J. (2015-07-01). "Fructose-containing sugars and cardiovascular disease". Advances in Nutrition (Bethesda, Md.). 6 (4): 430–439. doi:10.3945/an.114.008177. ISSN 2156-5376. PMC 4496738. PMID 26178027.
- 1 2 3 EFSA Panel on Dietetic Products, Nutrition and Allergies (2011). "Scientific Opinion on the substantiation of health claims related to fructose and reduction of post-prandial glycaemic responses (ID 558) pursuant to Article 13(1) of Regulation (EC) No 1924/2006" (PDF). EFSA Journal. 9 (6): 2223. doi:10.2903/j.efsa.2011.2223.
- ↑ "Carbohydrates and Health" (PDF). UK Scientific Advisory Committee on Nutrition, Public Health England, TSO, Williams Lea, Norwich, UK. 2015. Retrieved 1 April 2016.
- ↑ "Institute of Organic Chemistry".
- ↑ McWilliams, Margaret. Foods: Experimental Perspectives, 4th Edition. ISBN 0-13-021282-2.
- ↑ Keusch, P. "Yeast and Sugar- the Chemistry must be right". Archived from the original on December 20, 2010.
- ↑ Dills, WL (1993). "Protein fructosylation: Fructose and the Maillard reaction". Journal of Clinical Nutrition. 58: 779–787.
- ↑ Huber, G. W.; Iborra, S.; Corma, A. Chem. Rev. 2006, 106, 4044 – 4098. doi:10.1021/cr068360d
- 1 2 3 4 5 Hanover, LM; White, JS (1993). "Manufacturing, composition, and application of fructose". Journal of Clinical Nutrition. 58: 724s–732.
- ↑ Oregon State University. "Sugar Sweetness". Last accessed May 5, 2008. http://food.oregonstate.edu/sugar/sweet.html Archived May 16, 2008, at the Wayback Machine.
- ↑ Shallenberger, R.S. (1994). Taste Chemistry. Chapman and Hall. ISBN 978-0-7514-0150-9.
- 1 2 Nabors, LO (2001). "American Sweeteners": 374–375.
- ↑ McWilliams, Margaret (2001). Foods: Experimental Perspectives, 4th Edition. Upper Saddle River, NJ : Prentice Hall. ISBN 0-13-021282-2.
- ↑ White, DC; Lauer GN (1990). "Predicting gelatinization temperature of starch/sweetener system for cake formulation by differential scanning calorimetry I. Development of a model". Cereal Foods World. 35: 728–731.
- ↑ Margaret M. Wittenberg (2007). New Good Food: Essential Ingredients for Cooking and Eating Well. Diet and Nutrition Series; pages 249-51. Ten Speed Press. ISBN 1580087507.
- ↑ Park, KY; Yetley AE (1993). "Intakes and food sources of fructose in the United States". American Journal of Clinical Nutrition. 58 (5 Suppl): 737S–747S. PMID 8213605.
- ↑ Riby, JE; Fujisawa T; Kretchmer N (1993). "Fructose absorption". American Journal of Clinical Nutrition. 58 (5 Suppl): 748S–753S. PMID 8213606.
- 1 2 3 Kretchmer, N; Hollenbeck CB (1991). "Sugars and Sweeteners". CRC Press, Inc.
- 1 2 "Search the USDA National Nutrient Database for Standard Reference". Nal.usda.gov. Retrieved 10 December 2014.
- ↑ John S White, Straight talk about high-fructose corn syrup, The American Journal of Clinical Nutrition, 2008
- ↑ Guthrie, FJ; Morton FJ (2000). "Food sources of added sweeteners in the diets of Americans". Journals of American Dietetic Association. 100: 43–51. doi:10.1016/S0002-8223(00)00018-3.
- ↑ Stipanuk, Marsha H (2006). "Biochemical, Physiological, and Molecular Aspects of Human Nutrition, 2nd Edition". W.B. Saunders, Philadelphia, PA.
- 1 2 Fujisawa, T; Riby J; Kretchmer N (1991). "Intestinal absorption of fructose in the rat". Gastroenterology. 101 (2): 360–367. PMID 2065911.
- ↑ Ushijima, K; Fujisawa T; Riby J; Kretchmer N (1991). "Absorption of fructose by isolated small intestine of rats is via a specific saturable carrier in the absence of glucose and by the disaccharidase-related transport system in the presence of glucose". Journal of Nurtition. 125 (8): 2156–2164. PMID 7643250.
- ↑ Ferraris, R (2001). "Dietary and developmental regulation of intestinal sugar transport". Journal of Biochemistry. 360 (Pt 2): 265–276. doi:10.1042/0264-6021:3600265. PMC 1222226. PMID 11716754.
- 1 2 Beyer, PL; Caviar EM; McCallum RW (2005). "Fructose intake at current levels in the United States may cause gastrointestinal distress in normal adults". J. Am. Diet. Assoc. 105 (10): 1559–1566. doi:10.1016/j.jada.2005.07.002. PMID 16183355.
- ↑ Ravich, WJ; Bayless TM; Thomas, M (1983). "Fructose: incomplete intestinal absorption in humans". Gastroenterology. 84 (1): 26–29. PMID 6847852.
- ↑ Riby, JE; Fujisawa T; Kretchmer, N (1993). "Fructose absorption". American Journal of Clinical Nutrition. 58 (5 Suppl): 748S–753S. PMID 8213606.
- ↑ Rumessen, JJ; Gudman-Hoyer E (1986). "Absorption capacity of fructose in healthy adults. Comparison with sucrose and its constituent monosaccharides". Gut. 27 (10): 1161–1168. doi:10.1136/gut.27.10.1161. PMC 1433856. PMID 3781328.
- ↑ Skoog, SM; Bharucha AE (2004). "Dietary fructose and gastrointestinal symptoms: a review". Am. J. Gastroenterol. 99 (10): 2046–50. doi:10.1111/j.1572-0241.2004.40266.x. PMID 15447771.
- ↑ Fujisawa, T, T; Mulligan K; Wada L; Schumacher L; Riby J; Kretchmer N (1993). "The effect of exercise on fructose absorption". Am. J. Clin. Nutr. 58 (1): 75–9. PMID 8317393.
- ↑ Quezada-Calvillo, R; Robayo CC; Nichols BL (2006). Carbohydrate Digestion and Absorption. Missouri: Saunders, Elsevier. pp. 182–185. ISBN 1-4160-0209-X.
- ↑ Hajduch, E; Litherland GJ; Turban S; Brot-Laroche E; Hundal HS (Aug 2003). "Insulin regulates the expression of the GLUT5 transporter in L6 skeletal muscle cells". FEBS Letters. 549 (1–3): 77–82. doi:10.1016/S0014-5793(03)00773-7. PMID 12914929.
- ↑ MA Parniak; Kalant N (1988). "Enhancement of glycogen concentrations in primary cultures of rat hepatocytes exposed to glucose and fructose". Biochemical Journal. 251 (3): 795–802. doi:10.1042/bj2510795. PMC 1149073. PMID 3415647.
- 1 2 McGrane, MM (2006). Carbohydrate metabolism: Synthesis and oxidation. Missouri: Saunders, Elsevier. pp. 258–277. ISBN 1-4160-0209-X.
- 1 2 Sul, HS (2006). Metabolism of Fatty Acids, Acylglycerols, and Sphingolipids. Missouri: Saunders, Elsevier. pp. 450–467. ISBN 1-4160-0209-X.
- ↑ Buchs, AE; Sasson S; Joost HG; Cerasi E. (1998). "Characterization of GLUT5 domains responsible for fructose transport". Endocrinology. 139 (3): 827–31. doi:10.1210/en.139.3.827. PMID 9492009.
- ↑ Kwon, Oran; et al. (22 September 2007). "Inhibition of the intestinal glucose transporter GLUT2 by flavonoids" (PDF). FASEB Journal. 21 (2): 366–377. doi:10.1096/fj.06-6620com. PMID 17172639.
- ↑ Eswaran, Shanti; Tack, Jan; Chey, William D. (2011-03-01). "Food: the forgotten factor in the irritable bowel syndrome". Gastroenterology Clinics of North America. 40 (1): 141–162. doi:10.1016/j.gtc.2010.12.012. ISSN 1558-1942. PMID 21333905.
- 1 2 DiNicolantonio, James J.; Lucan, Sean C. "Is fructose malabsorption a cause of irritable bowel syndrome?". Medical Hypotheses. 85 (3): 295–297. doi:10.1016/j.mehy.2015.05.019. PMC 4729202. PMID 26059250.
- ↑ Sievenpiper JL, de Souza RJ, Mirrahimi A, Yu ME, Carleton AJ, Beyene J, Chiavaroli L, Di Buono M, Jenkins AL, Leiter LA, Wolever TM, Kendall CW, Jenkins DJ (Feb 21, 2012). "Effect of Fructose on Body Weight in Controlled Feeding Trials: A Systematic Review and Meta-analysis". Ann Intern Med. 156 (4): 291–304. doi:10.7326/0003-4819-156-4-201202210-00007. PMID 22351714.
- 1 2 Regnault, Timothy R. H.; Gentili, Sheridan; Sarr, Ousseynou; Toop, Carla R.; Sloboda, Deborah M. (2013-11-01). "Fructose, pregnancy and later life impacts". Clinical and Experimental Pharmacology & Physiology. 40 (11): 824–837. doi:10.1111/1440-1681.12162. ISSN 1440-1681. PMID 24033459.
- ↑ Lustig RH (2006). "Childhood obesity: behavioral aberration or biochemical drive? Reinterpreting the First Law of Thermodynamics". Nature Clinical Practice Endocrinology & Metabolism. 2 (8): 447–58. doi:10.1038/ncpendmet0220. PMID 16932334.
- ↑ Bantle, J. P.; Raatz, S. K.; Thomas, W.; Georgopoulos, A. (2000-11-01). "Effects of dietary fructose on plasma lipids in healthy subjects". The American Journal of Clinical Nutrition. 72 (5): 1128–1134. ISSN 0002-9165. PMID 11063439.
- ↑ Rippe, J. M.; Angelopoulos, T. J. (2015). "Fructose-Containing Sugars and Cardiovascular Disease". Advances in Nutrition. 6 (4): 430–439. doi:10.3945/an.114.008177. ISSN 2156-5376. PMC 4496738. PMID 26178027.
- ↑ Brown, C. M.; Dulloo, A. G.; Montani, J.-P. (2008-12-01). "Sugary drinks in the pathogenesis of obesity and cardiovascular diseases". International Journal of Obesity (2005). 32 Suppl 6: S28–34. doi:10.1038/ijo.2008.204. ISSN 1476-5497. PMID 19079277.
- ↑ Jalal, Diana I.; Smits, Gerard; Johnson, Richard J.; Chonchol, Michel (2010-09-01). "Increased Fructose Associates with Elevated Blood Pressure". Journal of the American Society of Nephrology. 21 (9): 1543–1549. doi:10.1681/ASN.2009111111. ISSN 1046-6673. PMC 3013529. PMID 20595676.
- ↑ Bray, George A. (2013-03-01). "Energy and fructose from beverages sweetened with sugar or high-fructose corn syrup pose a health risk for some people". Advances in Nutrition (Bethesda, Md.). 4 (2): 220–225. doi:10.3945/an.112.002816. ISSN 2156-5376. PMC 3649102. PMID 23493538.
- ↑ Perlstein, Todd S.; Gumieniak, Olga; Williams, Gordon H.; Sparrow, David; Vokonas, Pantel S.; Gaziano, Michael; Weiss, Scott T.; Litonjua, Augusto A. (2006-12-01). "Uric acid and the development of hypertension: the normative aging study". Hypertension. 48 (6): 1031–1036. doi:10.1161/01.HYP.0000248752.08807.4c. ISSN 1524-4563. PMID 17060508.
- ↑ Hallfrisch, J. (1990-06-01). "Metabolic effects of dietary fructose". FASEB Journal. 4 (9): 2652–2660. ISSN 0892-6638. PMID 2189777.
- ↑ Truswell AS (1994). "Food carbohydrates and plasma lipids--an update" (PDF). Am J Clin Nutr. Am Soc Clin Nutr. 59 (3(Suppl)): 710S–718S. PMID 8116555. Retrieved 31 July 2012.
- ↑ Bantle JP, Raatz SK, Thomas W, Georgopoulos A (2000). "Effects of dietary fructose on plasma lipids in healthy subjects". Am. J. Clin. Nutr. 72 (5): 1128–34. PMID 11063439.
- ↑ Stanhope, Kimber L.; Medici, Valentina; Bremer, Andrew A.; Lee, Vivien; Lam, Hazel D.; Nunez, Marinelle V.; Chen, Guoxia X.; Keim, Nancy L.; Havel, Peter J. (2015-06-01). "A dose-response study of consuming high-fructose corn syrup-sweetened beverages on lipid/lipoprotein risk factors for cardiovascular disease in young adults". The American Journal of Clinical Nutrition. 101 (6): 1144–1154. doi:10.3945/ajcn.114.100461. ISSN 1938-3207. PMC 4441807. PMID 25904601.
- ↑ A. M. Grant; M. R. Christie; S. J. Ashcroft (August 1980). "Insulin Release from Human Pancreatic Islets in Vitro". Diabetologia. 19 (2): 114–117. doi:10.1007/BF00421856. PMID 6998814.
- ↑ D. L. Curry (1989). "Effects of Mannose and Fructose on the Synthesis and Secretion of Insulin". Pancreas. 4 (1): 2–9. doi:10.1097/00006676-198902000-00002. PMID 2654926.
- ↑ Y. Sato; T. Ito; N. Udaka; et al. (December 1996). "Immunohistochemical Localization of Facilitated-Diffusion Glucose Transporters in Rat Pancreatic Islets". Tissue Cell. 28 (6): 637–643. doi:10.1016/S0040-8166(96)80067-X. PMID 9004533.
- ↑ "Fructose No Substitute for Glucose in Diabetes". Medpagetoday.com. 7 December 2011. Retrieved 10 December 2014.
- ↑ Kaye Foster-Powell; Susanna H. A. Holt; Janette C. Brand-Miller (2002). "International Table of Glycemic Index and Glycemic Load Values: 2002". American Journal of Clinical Nutrition. 76 (1): 5–56. PMID 12081815.
- ↑ Patricia M. Heacock; Steven R. Hertzler; Bryan W. Wolf (2002). "Fructose Prefeeding Reduces the Glycemic Response to a High-Glycemic Index, Starchy Food in Humans". Journal of Nutrition. 132 (9): 2601–2604. PMID 12221216.
- ↑ Ouyang X; Cirillo P; Sautin Y; et al. (June 2008). "Fructose Consumption as a Risk Factor for Non-alcoholic Fatty Liver Disease". J. Hepatol. 48 (6): 993–9. doi:10.1016/j.jhep.2008.02.011. PMC 2423467. PMID 18395287.
- ↑ Abid A, Taha O, Nseir W, Farah R, Grosovski M, Assy N (November 2009). "Soft drink consumption is associated with fatty liver disease independent of metabolic syndrome". Journal of Hepatology. 51 (5): 918–24. doi:10.1016/j.jhep.2009.05.033. PMID 19765850. Cited in review article: Machado MV, Cortez-Pinto H (September 2014). "Non-alcoholic fatty liver disease: What the clinician needs to know". World Journal of Gastroenterology : WJG. 20 (36): 12956–12980. doi:10.3748/wjg.v20.i36.12956. PMC 4177476. PMID 25278691.
- ↑ Choi, Hyon K.; Curhan, Gary. "Soft drinks, fructose consumption, and the risk of gout in men: prospective cohort study". BMJ. Retrieved 5 December 2011.
- ↑ Teff, KL; Elliott SS; Tschöp M; Kieffer TJ; Rader D; Heiman M; Townsend RR; Keim NL; D'Alessio D; Havel PJ (June 2004). "Dietary fructose reduces circulating insulin and leptin, attenuates postprandial suppression of ghrelin, and increases triglycerides in women". J Clin Endocrinol Metab. 89 (6): 2963–72. doi:10.1210/jc.2003-031855. PMID 15181085.
- ↑ Swan, Norman; Lustig, Robert H. "ABC Radio National, The Health Report, The Obesity Epidemic". Retrieved 2007-07-15.
External links
Sugar (as food commodity) | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
List of sugars and sugar products | |||||||||||
| Chemistry |  | ||||||||||
| Sources | |||||||||||
| Products |
| ||||||||||
| Industry |
| ||||||||||
| History | |||||||||||
| Culture | |||||||||||
| Related | |||||||||||
| |||||||||||