Balo concentric sclerosis
| Balo concentric sclerosis | |
|---|---|
|
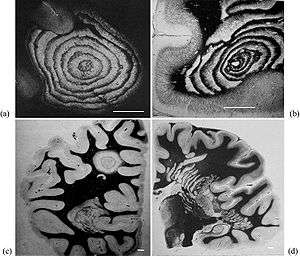
Typical aspects of Baló's concentric sclerosis. (a) Original case of Baló; several anastomoses are located in the lower half of the lesion. (b) Lesion centered by a veinule showing ring fragmentation in a constrained area. (c) Lesion. (d) Progress of the pathologic process from a center located in a constrained area, showing formation of bands. Loyez staining (myelin in black, destroyed areas in white); scale bars: 1 cm. | |
| Classification and external resources | |
| Specialty | neurology |
| ICD-10 | G37.5 |
| ICD-9-CM | 341.1 |
| DiseasesDB | 11849 |
| MeSH | D002549 |
Balo concentric sclerosis is a disease in which the white matter of the brain appears damaged in concentric layers, leaving the axis cylinder intact.[1] It was described by Joszef Balo who initially named it "leuko-encephalitis periaxialis concentrica" from the previous definition,[2] and it is currently considered one of the borderline forms of multiple sclerosis.
Balo concentric sclerosis is a demyelinating disease similar to standard multiple sclerosis, but with the particularity that the demyelinated tissues form concentric layers. Scientists used to believe that the prognosis was similar to Marburg multiple sclerosis, but now they know that patients can survive, or even have spontaneous remission and asymptomatic cases.[3]
It is also common that the clinical course is primary progressive, but a relapsing-remitting course has been reported.[4] It seems that the course gets better with prednisone therapy,[5] although evidence of this is anecdotal and such conclusions are difficult to accept given that there are cases where patients spontaneously recover whether the patient was on steroid therapy or not.
Pathophysiology
The lesions of the Balo sclerosis belong to the MS lesion pattern III (distal oligodendrogliopathy).[6] Balo concentric sclerosis is now believed to be a variant of pattern III multiple sclerosis.[7]
According with Dr. Lucchinetti investigations, in Balo's concentric sclerosis, the rings may be caused by a physiological hypoxia (similar to that caused by some toxins or viruses) in the lesion, which is in turn countered by expression of stress proteins at the border. This expression and counter-expression forms rings of preserved tissue within the lesion and rings of demyelinated tissue just beyond where the previous attack had induced the protective stress proteins. Hence, subsequent attacks form concentric rings.[8]
Some other researchers maintain that, as in pattern III MS, the mitochondrial respiratory chain complex IV activity is reduced and this could be the culprit of glutamate-mediated axonal injury.[9]
Other two propossed mechanisms are the presence of granulation tissue in old lesions, which is rich in capillaries and could act as an energy reservoir, and the small adherent bands of myelinated tissue. These two mechanisms are proposed based in the assumption of a hypoxic causation principle[10]
Ultimately, this expanding lesion causes the progressive picture typically seen. However, in some patients, the pathology underlying the disease appears to burn out and hence the disease may halt, hence the patients who spontaneously recover. The mechanisms triggering attacks and recovery remain uncertain.
Nevertheless, this model is questioned by recent reports that found astrocyte damage, similar to the one found in aquaporin-seropositive neuromyelitis optica. Though no anti-NMO antibodies have been found, the damage is similar, pointing to problems in the water channel of the astrocytes[11][12]
It presents three clinical subtypes: Monophasic, relapsing-remitting and primary rapidly progressive. CSF is either normal or shows mild mononuclear inflammatory reaction. Oligoclonal bands are present only in few cases[13]
Lesions under MRI
The features of the MRI and the characteristics of the lesion can be correlated when a biopsy has been taken, providing a way to standarize the future MRI diagnosis[14]
Balo concentric sclerosis lesions can be distinguished from normal lesions on MRI showing alternative hypotense and hypertense layers[15]
Balo concentric lesions can be viewed using the myelin water imaging techniques. This is a special MRI sequence that shows the myelin's percentage of water content.[16]
Models
A mathematical model for concentric sclerosis has been proposed.[17] Authors review the previous pathogenic theories, discuss the link between concentric sclerosis and Liesegang's periodic precipitation phenomenon and propose a new mechanism based on self-organization.
Spectrum
Balo lesions have been reported alone, but also associated to standard multiple sclerosis, neuromyelitis optica, CADASIL and progressive multifocal leukoencephalopathy[18]
Paediatric cases
Balo concentric sclerosis in children has been reported to behave different from adults[19]
Lesions in autopsy and biopsy
A report comparing 1H-magnetic resonance spectroscopy, magnetization transfer and diffusion tensor imaging with histopathology in a patient with Balo's concentric sclerosis, found that inflammation was traced by fractional anisotropy and increased lactate. In contrast, magnetization transfer ratio and the diffusion coefficient show a loss of tissue in the rings of the lesion.[20]
Epidemiology
The disease is more common in Chinese and Filipino populations (both Asiatic) than in caucasoids.[21]
History
Though the disease carries the name of Joszef Balo, it was first described by Otto Marburg in 1906[22] Later, in 1928, Joszef Balo studied the encephalitis periaxialis concentrica in a Hungarian patient, showing also demyelination of the peripheral nervous system.
See also
References
- ↑ Balo J (1928). "Encephalitis periaxialis concentrica". Arch Neurol Psychiatry. 19: 242–244. doi:10.1001/archneurpsyc.1928.02210080044002.
- ↑ Purohit; et al. (2015). "Balo's Concentric Sclerosis with Acute Presentation and Co-Existing Multiple Sclerosis-Typical Lesions on MRI". Case Rep Neurol. 7 (1): 44–50. doi:10.1159/000380813.
- ↑ Karaarslan E, Altintas A, Senol U, et al. (August 2001). "Baló's concentric sclerosis: clinical and radiologic features of five cases". AJNR Am J Neuroradiol. 22 (7): 1362–7. PMID 11498428.
- ↑ Moore GR, Berry K, Oger JJ, Prout AJ, Graeb DA, Nugent RA (December 2001). "Baló's concentric sclerosis: surviving normal myelin in a patient with a relapsing-remitting dinical course". Mult. Scler. 7 (6): 375–82. doi:10.1177/135245850100700606. PMID 11795459.
- ↑ Garbern J, Spence AM, Alvord EC (December 1986). "Balo's concentric demyelination diagnosed premortem". Neurology. 36 (12): 1610–4. doi:10.1212/WNL.36.12.1610. PMID 3785678.
- ↑ (Article in Spanish)
- ↑ Bogdan F. Popescu, MD, Istvan Pirko, and Claudia F. Lucchinetti, Pathology of Multiple Sclerosis: Where Do We Stand? Continuum (Minneap Minn). 2013 Aug; 19(4 Multiple Sclerosis): 901–921, PMCID:PMC3915566, doi:http://doi.org/10.1212/01.CON.0000433291.23091.65
- ↑ Genetic susceptibility in MS – Steve Hauser. Rare Neuroimmunologic Disorders Symposium
- ↑ Don J. Mahad, Iryna Ziabreva, Graham Campbell, Nichola Lax, Katherine White, Peter S. Hanson, Hans Lassmann, Douglass M. Turnbull, Mitochondrial changes within axons in multiple sclerosis, DOI: http://dx.doi.org/10.1093/brain/awp046, 17 March 2009
- ↑ Helmut Barza, b, , Ulrich Barzc, Almut Schreiberd, Morphogenesis of the demyelinating lesions in Baló’s concentric sclerosis, Medical Hypotheses, Volume 91, June 2016, Pages 56–61, http://dx.doi.org/10.1016/j.mehy.2016.03.016
- ↑ Matsuoka Takeshi; et al. (Nov 2010). "Aquaporin-4 astrocytopathy in Baló's disease". Acta Neuropathol. 120 (5): 651–60. doi:10.1007/S00401-010-0733-7.
- ↑ Kira J (Jul 2011). "Astrocytopathy in Balo's disease". Mult Scler. 17 (7): 771–9. doi:10.1177/1352458511400475. PMID 21459811.
- ↑ Saeed Arif et al, ONION PEEL APPEARANCE IN BALOS CONCENTRIC SCLEROSIS, A VARIANT OF MULTIPLE SCLEROSIS, J Ayub Med Coll Abbottabad 2015;27(1)
- ↑ Darke, Bahador, Miller, Litofsky, Ahsan. Baló's concentric sclerosis: imaging findings and pathological correlation, J Radiol Case Rep. 2013 Jun 1;7(6):1-8. doi: 10.3941/jrcr.v7i6.1251. PMID 24421937
- ↑ IANNUCCI et al. Vanishing Balò-like lesions in multiple sclerosis, J Neurol Neurosurg Psychiatry 2000;69:399–400
- ↑ Cornelia Laule et al. Myelin water imaging of multiple sclerosis at 7 T: Correlations with histopathology, NeuroImage Volume 40, Issue 4, 1 May 2008, Pages 1575–1580, doi:10.1016/j.neuroimage.2007.12.008
- ↑ Khonsari RH, Calvez V (2007). Monk N, ed. "The Origins of Concentric Demyelination: Self-Organization in the Human Brain". PLoS ONE. 2 (1): e150. doi:10.1371/journal.pone.0000150. PMC 1764710
 . PMID 17225855.
. PMID 17225855. - ↑ Commentary on Pique et al.’s paper entitled: Peripheral late reactivation of a previously typical monofocal Balo’s concentric sclerosis lesion
- ↑ Linnoila J, Chitnis T (2014). "Balo Concentric Sclerosis in Children: A Case Series". J Child Neurol. 29 (5): 603–7. doi:10.1177/0883073813517294. PMID 24423690.
- ↑ Lindquist S (2007). "Histopathology and serial, multimodal magnetic resonance imaging in a multiple sclerosis variant". Mult Scler. 13 (4): 471–482.
- ↑ Article at mult-sclerosis.org
- ↑ Commentary on Pique et al.’s paper entitled: Peripheral late reactivation of a previously typical monofocal Balo’s concentric sclerosis lesion. Mult Scler July 2015 vol. 21 no. 8 1084-1086
Khonsari RH, Calvez V (September 2007). "Concentric demyelination by self-organization: a new hypothesis for Baló's sclerosis". Nat Clin Pract Neurol. 3 (9): E1. doi:10.1038/ncpneuro0619. PMID 17805242.